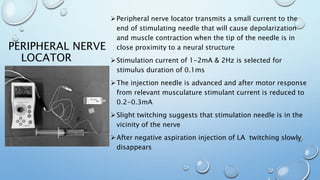
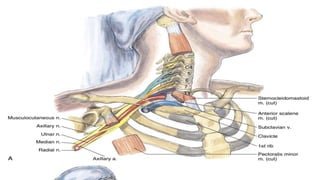
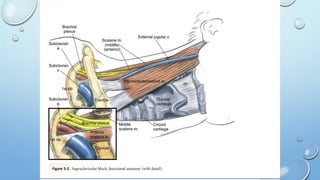
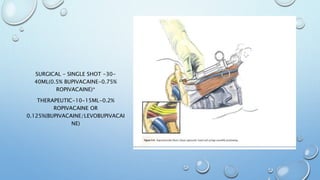
This document discusses regional blocks and pain medicine for the upper limb. It begins with a brief history of regional anesthesia techniques. It then describes various techniques including paresthesia, nerve stimulation, and ultrasound-guided blocks. Specific blocks covered include interscalene, supraclavicular, and intravenous regional anesthesia (Bier block). Advantages and disadvantages of each technique are provided. The document also discusses pharmacological considerations, contraindications, and complications of regional anesthesia in the upper limb.