Downloaded 176 times
![Airway solutions in an acute
trauma scenario
Dr.Venugopalan.P.P
DA;DNB;MNAMS;MEM[GWU]
Director ; Emergency Medicine
Aster DM Health Care Ltd
Deputy Director ;MIMS Academy
Founder and executive director -ANGELS](https://image.slidesharecdn.com/airwaysolutionsintraumascenarios-140928233513-phpapp01/75/Airway-solutions-in-trauma-scenarios-1-2048.jpg)









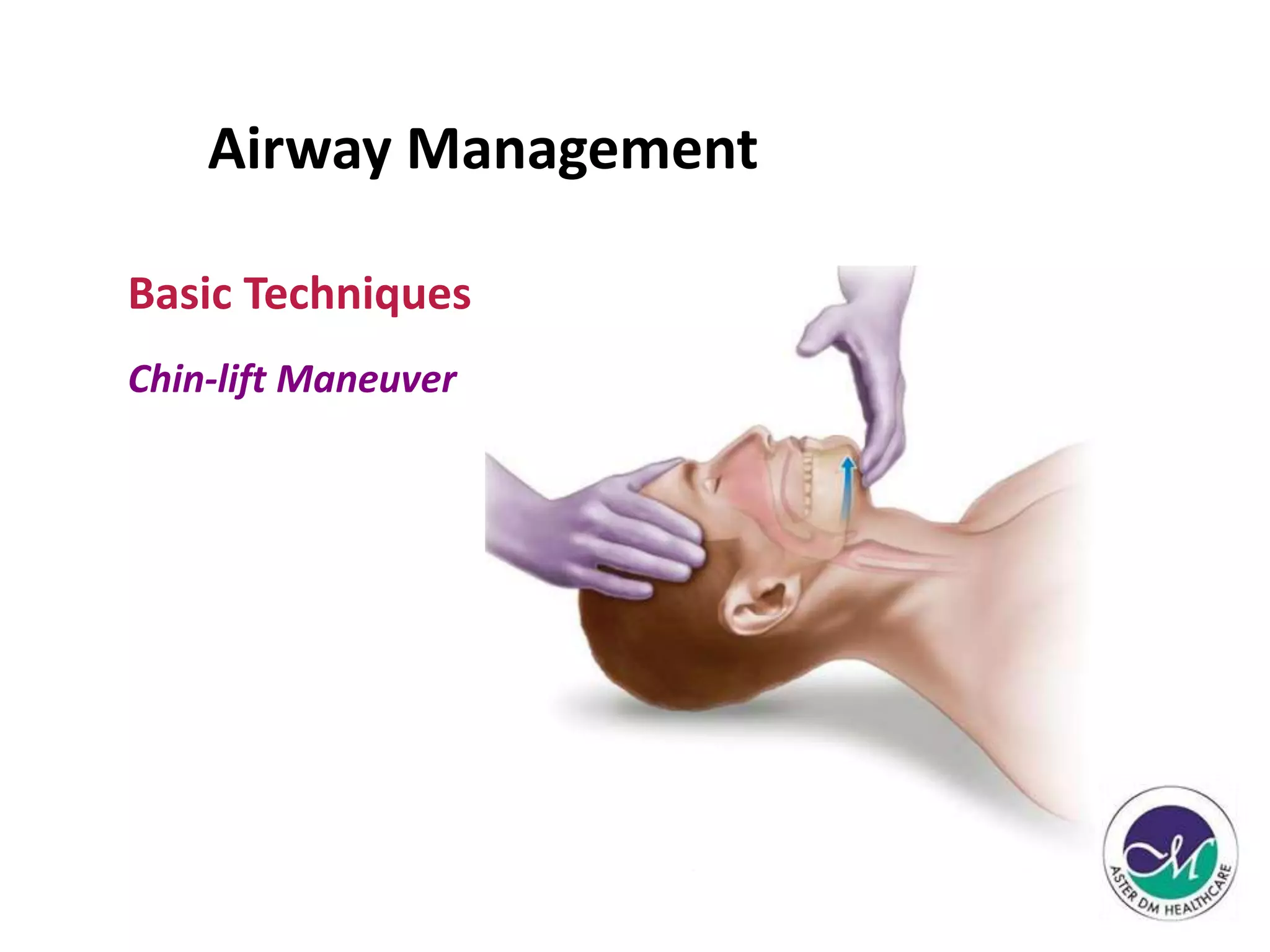



















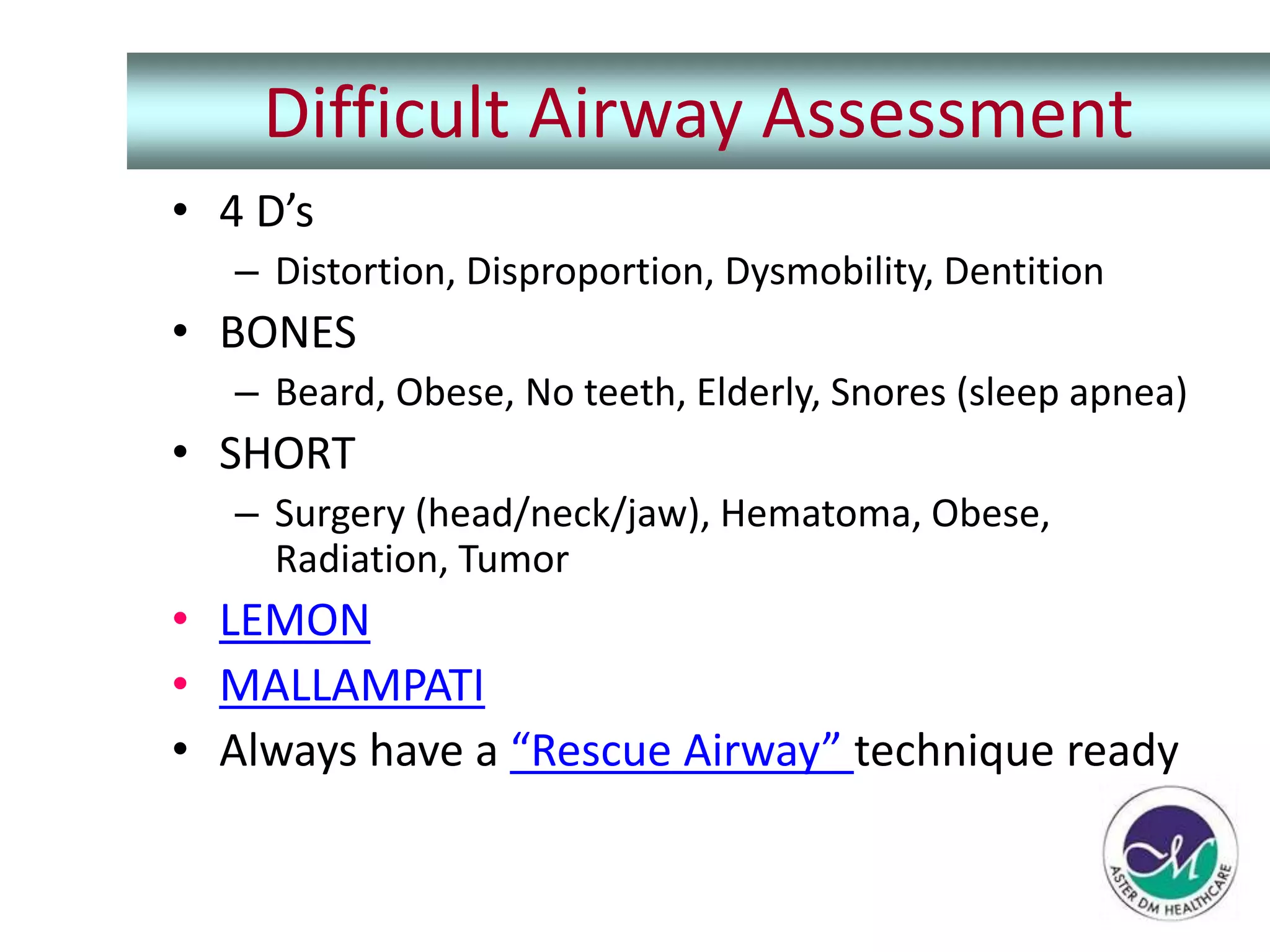
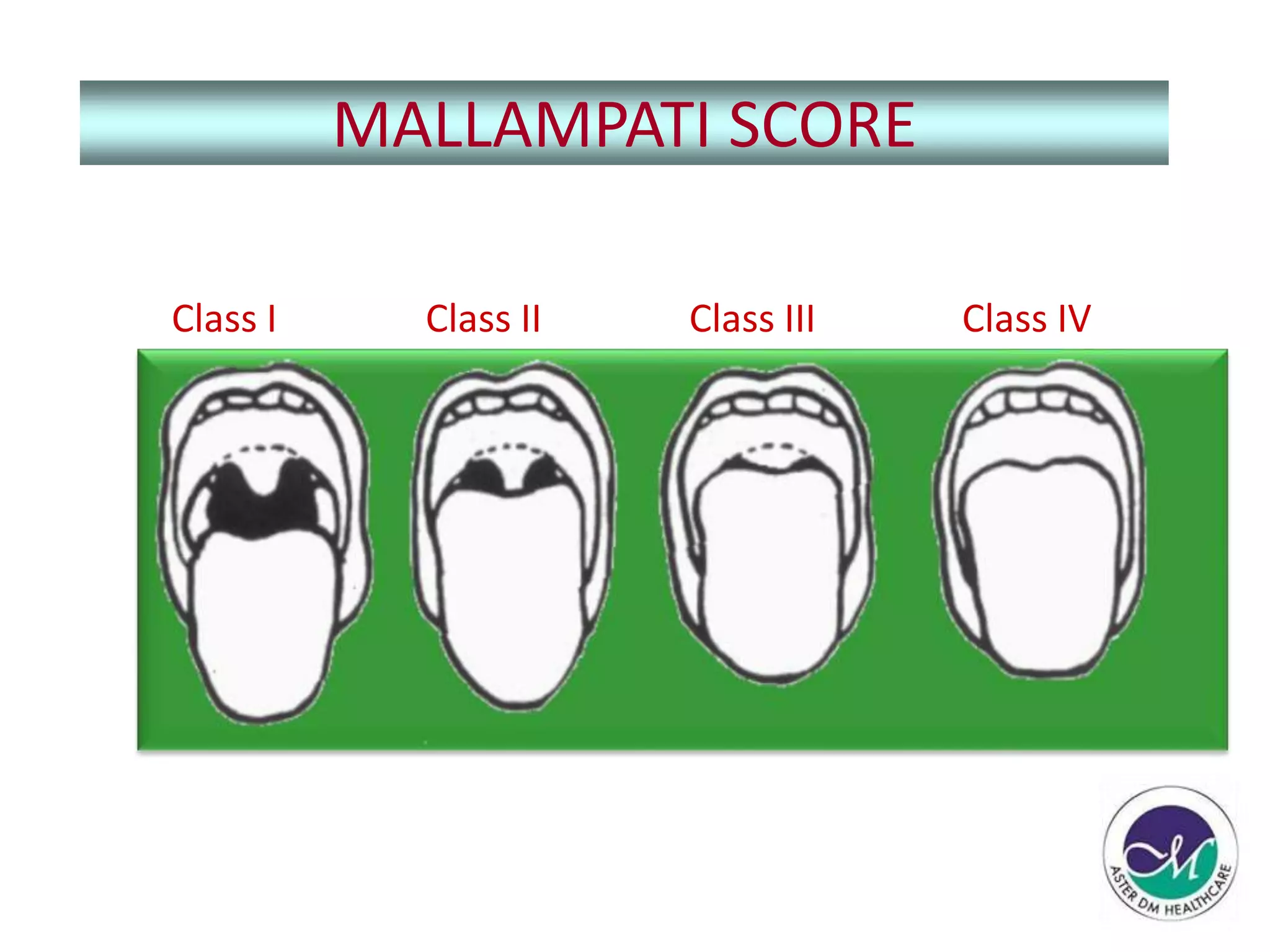



























1) The patient, a 28-year old man involved in a motorbike accident, has an impaired airway as evidenced by snoring, rapid breathing, and low oxygen saturation. 2) The top priority is securing the patient's airway. Basic airway maneuvers and adjuncts like chin lift, jaw thrust, oropharyngeal airway are appropriate first steps given intact reflexes. 3) If the airway cannot be maintained or there is impending compromise, more invasive techniques like intubation may be needed while protecting the cervical spine. Assessing risk factors can help predict difficult airways requiring specialized equipment or procedures like surgical airway.

























































![Anesthesia_for_Airway_management_and_Difficult_airway_Algorithmss[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforairwaymanagementanddifficultairwayalgorithmss11-250722203414-f94048f1-thumbnail.jpg?width=640&height=640&fit=bounds)

















































