Downloaded 662 times





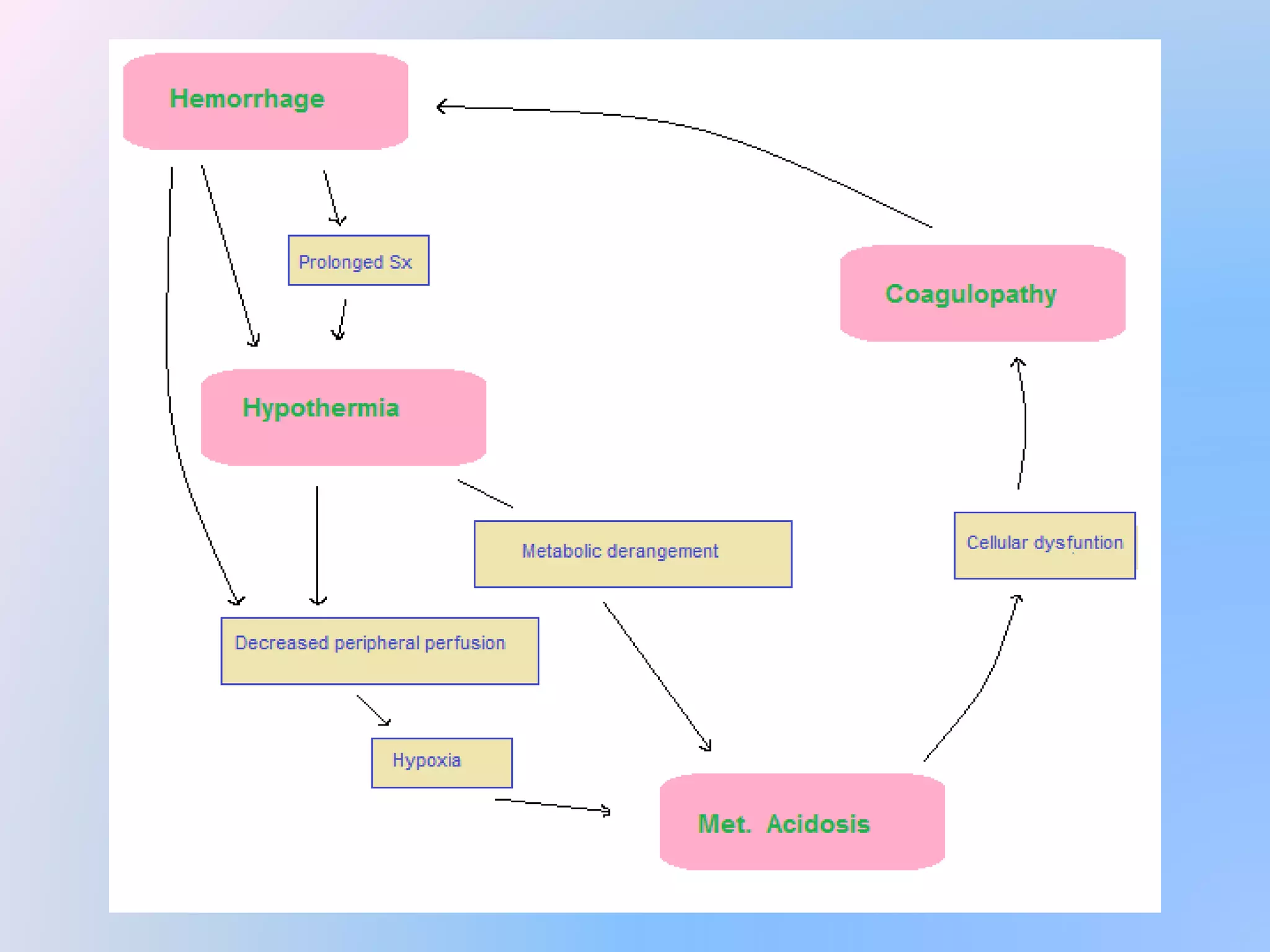












Damage control surgery (DCS) is an approach used for severely injured trauma patients that focuses on rapidly addressing life-threatening issues like hemorrhage rather than fully repairing anatomy. It aims to prevent the lethal triad of hypothermia, acidosis, and coagulopathy that can result from long operations and blood loss. Key aspects of DCS include temporary measures like packing bleeding liver injuries; stapling but not repairing some intestinal injuries; leaving unrepaired vascular injuries clamped; and rapidly closing the abdomen with clips rather than drains to allow reoperation once the patient is stabilized. The goal is definitive repair within 24 hours once the patient's physiology is corrected.























































































