Downloaded 340 times
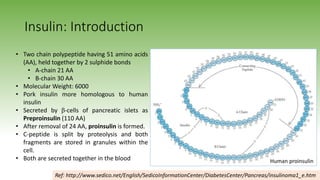
















1) Insulin is a polypeptide hormone composed of two chains that is secreted by the pancreas and regulates blood glucose levels. 2) Insulin secretion is regulated through chemical, hormonal, and neural mechanisms in response to glucose levels and other factors. It acts to promote glucose and lipid uptake and utilization and inhibits gluconeogenesis. 3) There are various insulin preparations including regular human insulin, lente/NPH insulin, and analogues like lispro, glargine, and detemir with different onset/duration profiles. Insulin is used to treat diabetes mellitus and diabetic ketoacidosis.











































































































