Downloaded 48 times
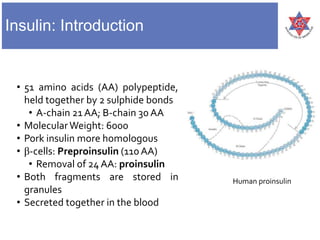
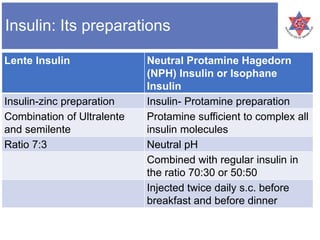

This document provides information about insulin, including: 1) It describes the structure of insulin as a 51 amino acid polypeptide made of an A-chain and B-chain, held together by disulfide bonds. 2) It explains that insulin secretion is regulated by both chemical and hormonal/neural mechanisms in response to glucose levels, including the roles of glucokinase and ATP-sensitive potassium channels. 3) It lists the different types of insulin preparations available, including regular insulin, NPH insulin, and rapid-acting insulin analogues like insulin lispro, aspart, and glulisine, as well as the long-acting insulin glargine and detemir.














































![INSULIN AND OTHER ANTIDIABETEC DRUGS [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/insulinandotherantidiabetecdrugsautosavedautosaved-220731124033-32b4f1bb-thumbnail.jpg?width=640&height=640&fit=bounds)








































