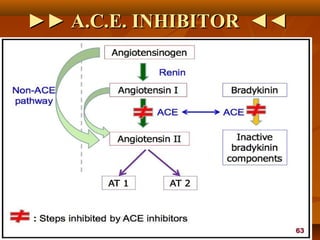
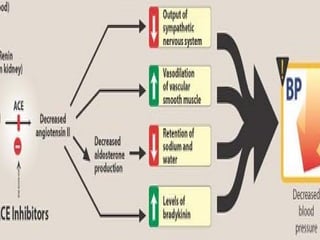
The document provides an overview of hypertension and classifications of antihypertensive drugs, focusing primarily on ACE inhibitors like captopril, enalapril, and ramipril. It details their mechanisms of action, therapeutic uses, side effects, contraindications, and pharmacokinetics. The document concludes with specific dosing recommendations and clinical uses for each ACE inhibitor.


































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




