Downloaded 237 times
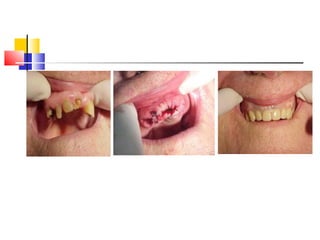
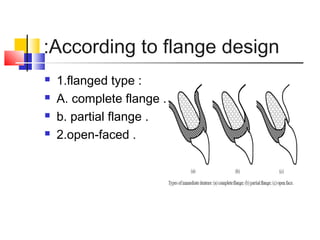

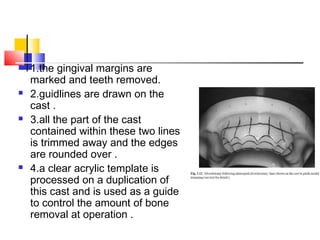
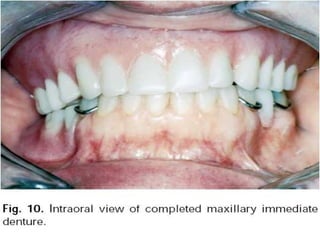


An immediate denture is a denture constructed before natural teeth are extracted, allowing it to be placed immediately after the extractions. It helps maintain appearance and functions like chewing and speech after tooth loss. While it provides advantages like minimized pain and bleeding, it also has limitations like inability to do try-ins and increased maintenance needs. The denture can be made with or without flanges, with flanged dentures providing better stability, strength and hemorrhage control but open-faced dentures may be preferable in cases with deep undercuts. Careful patient preparation and techniques like custom trays and records are needed to fabricate an immediate denture.





































































































