Downloaded 11 times

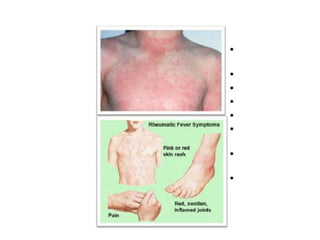
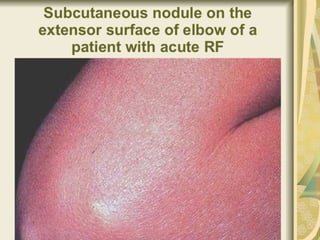
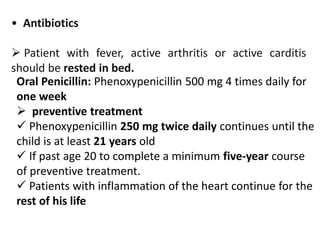
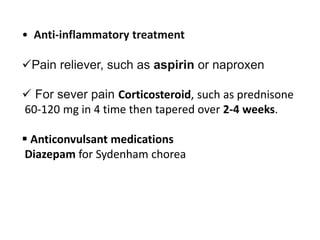
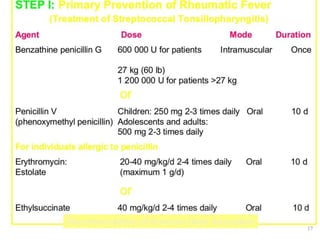


Rheumatic fever is most common in children aged 5 to 15 years and usually develops approximately 20 days after a streptococcal throat infection like strep throat or scarlet fever. It is caused by certain strains of streptococcus bacteria. Symptoms may include a bright red rash, sore throat, fever, and inflammation of the joints, heart, and brain. If left untreated, rheumatic fever can damage the heart valves and cause long-term problems. Treatment involves antibiotics to treat the initial strep infection as well as medications and rest to reduce inflammation and prevent long-term damage.











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





