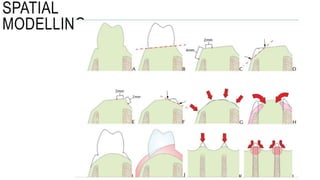
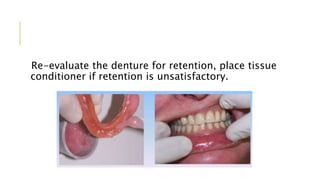
Immediate dentures are prostheses fabricated and inserted immediately following tooth extraction. There are two main types: conventional (classic) immediate dentures which serve as long-term prostheses, and interim (transitional) immediate dentures which will be replaced later after healing. The clinical and laboratory procedure involves making impressions, modifying the stone cast for improved fit, optionally using a surgical template, and inserting the denture immediately after extractions with follow-up relines and adjustments as needed. Immediate dentures can help maintain appearance, function, and quality of life but require more appointments and technical skill compared to delayed dentures.


















































![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)




















































