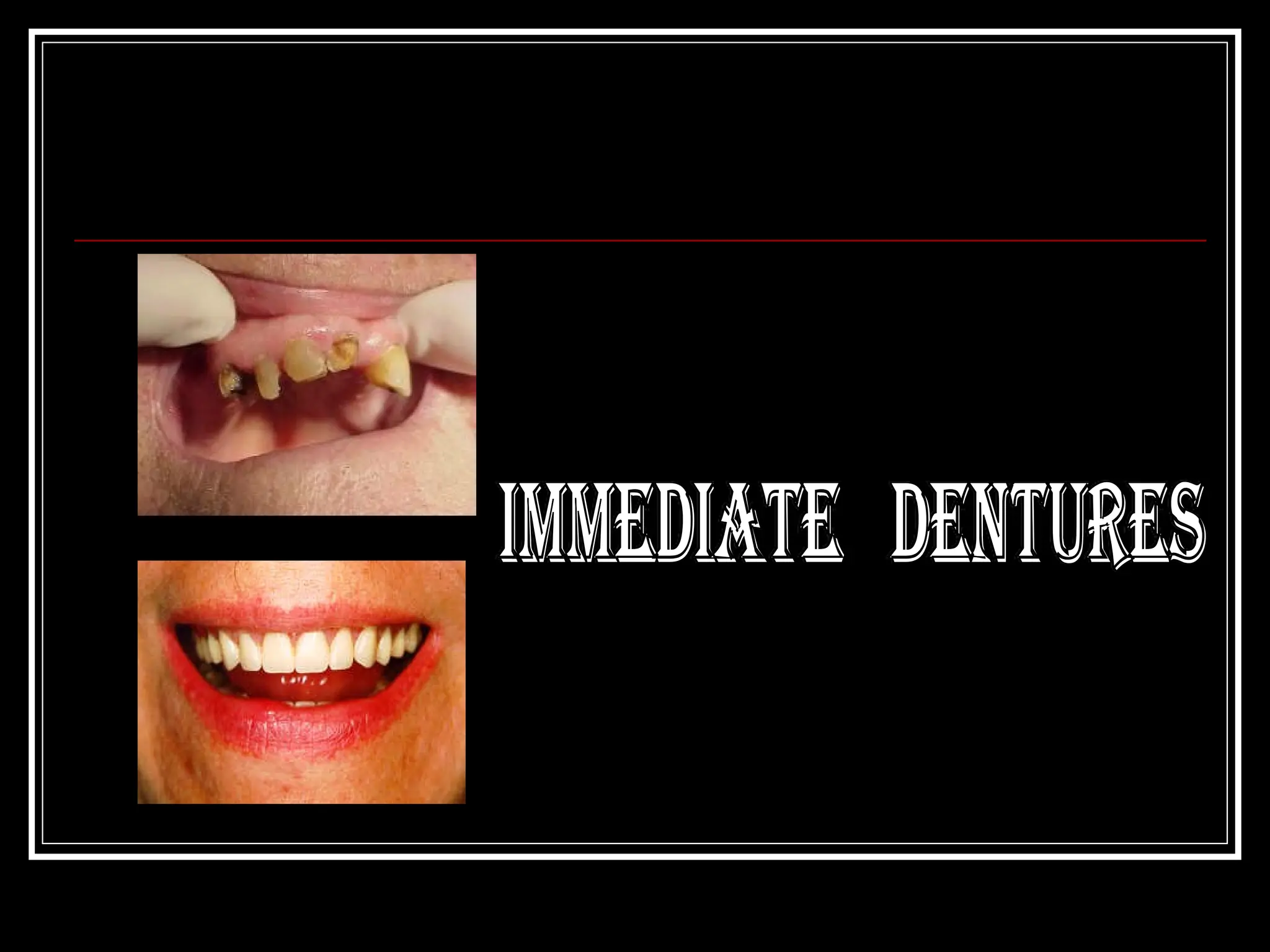
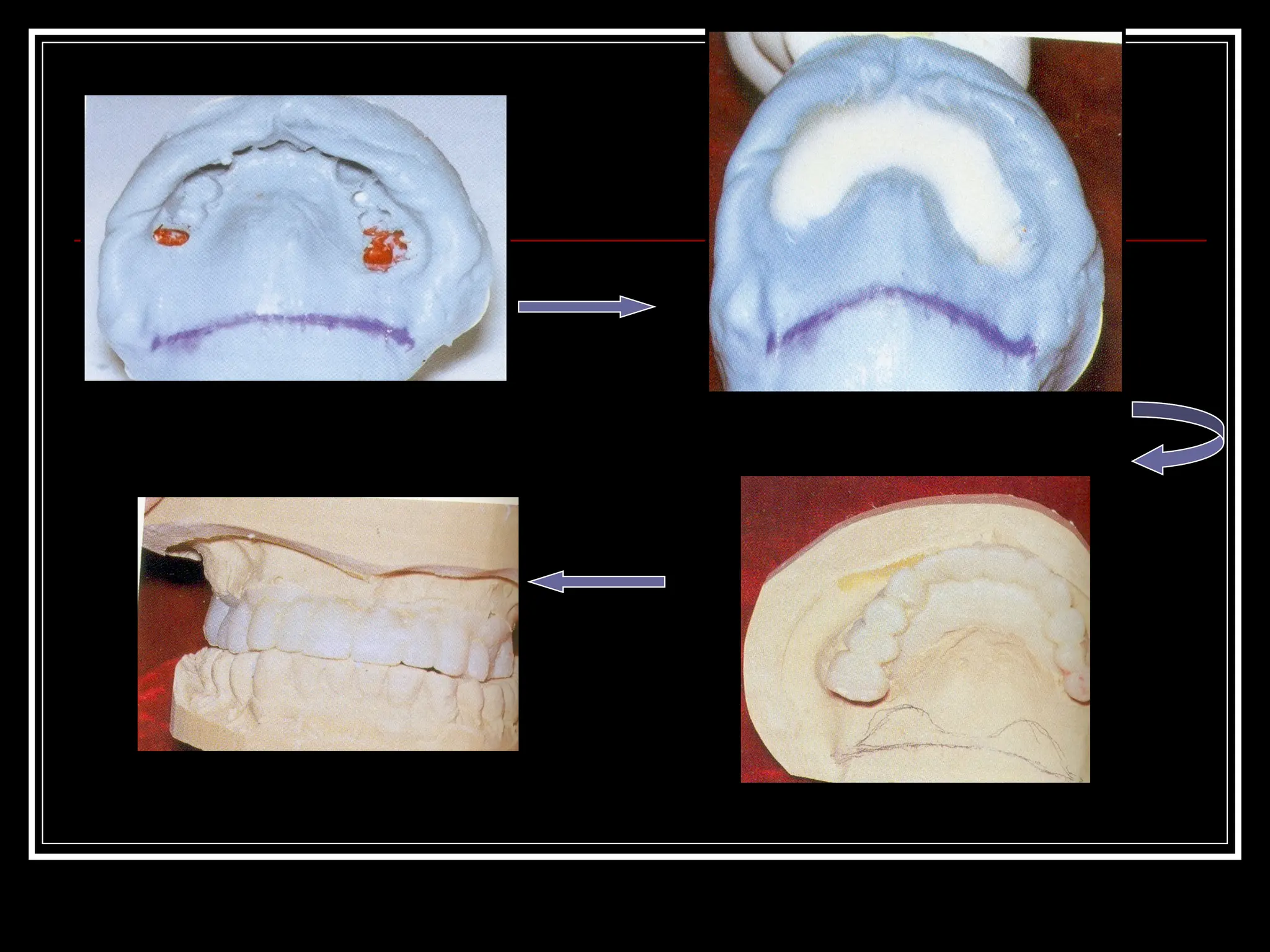
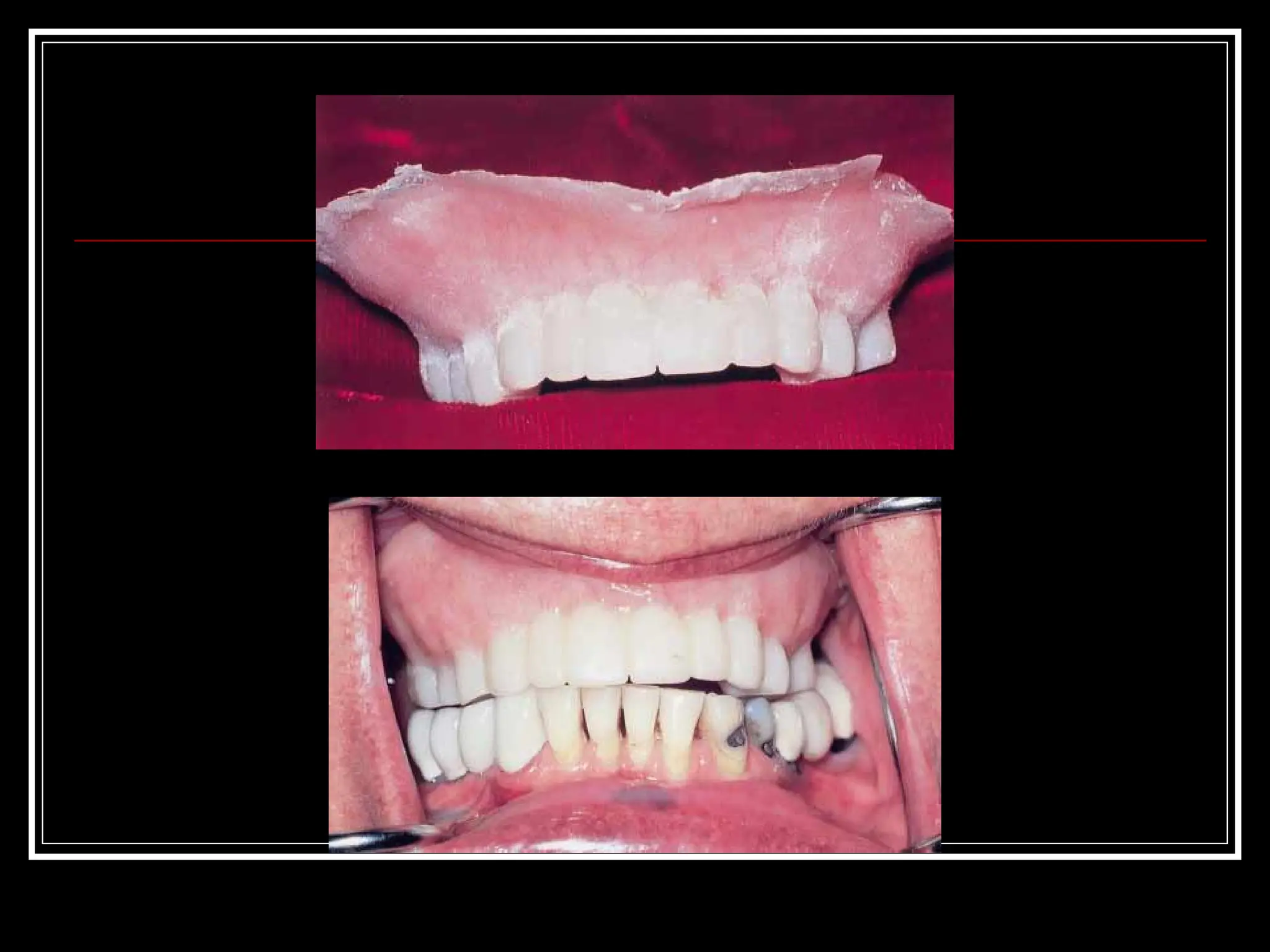
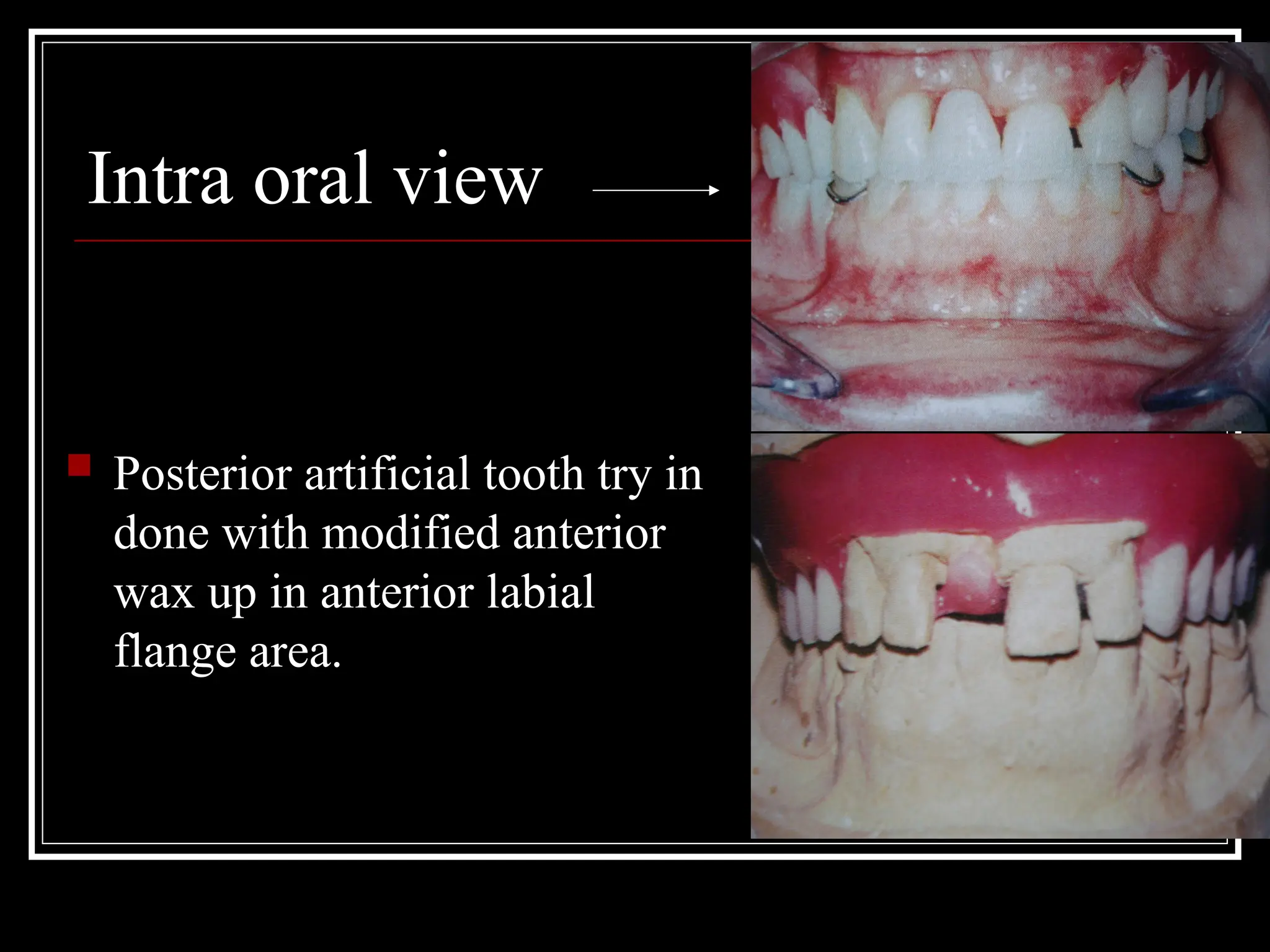
The document discusses immediate dentures, defined as prosthetic devices inserted immediately after tooth extraction to maintain appearance and function without edentulous periods. It outlines the advantages and disadvantages of immediate dentures, detailing the fabrication process, patient preparation, and care instructions. Literature references highlight techniques and considerations for successful immediate denture placement and patient outcomes.