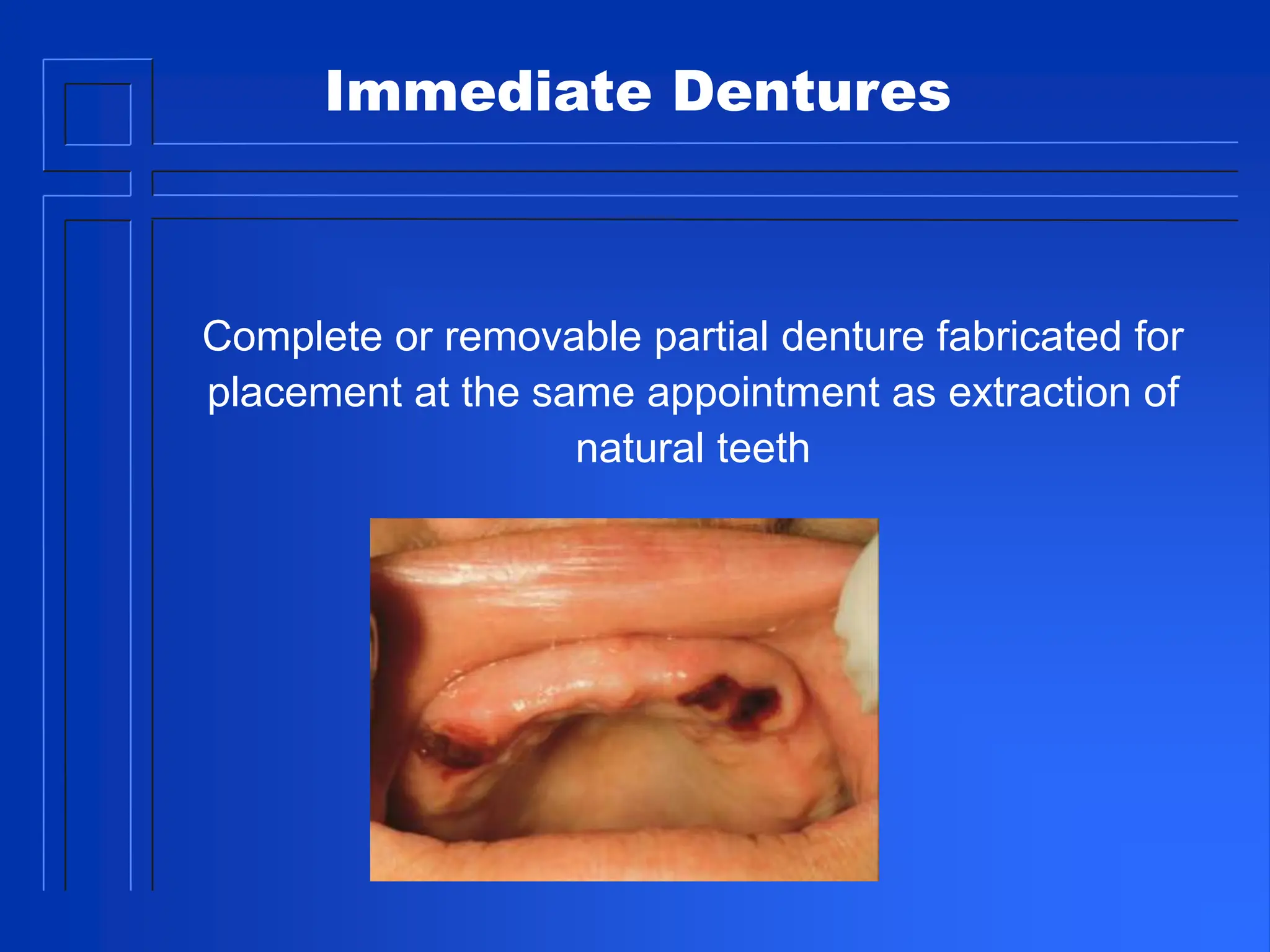
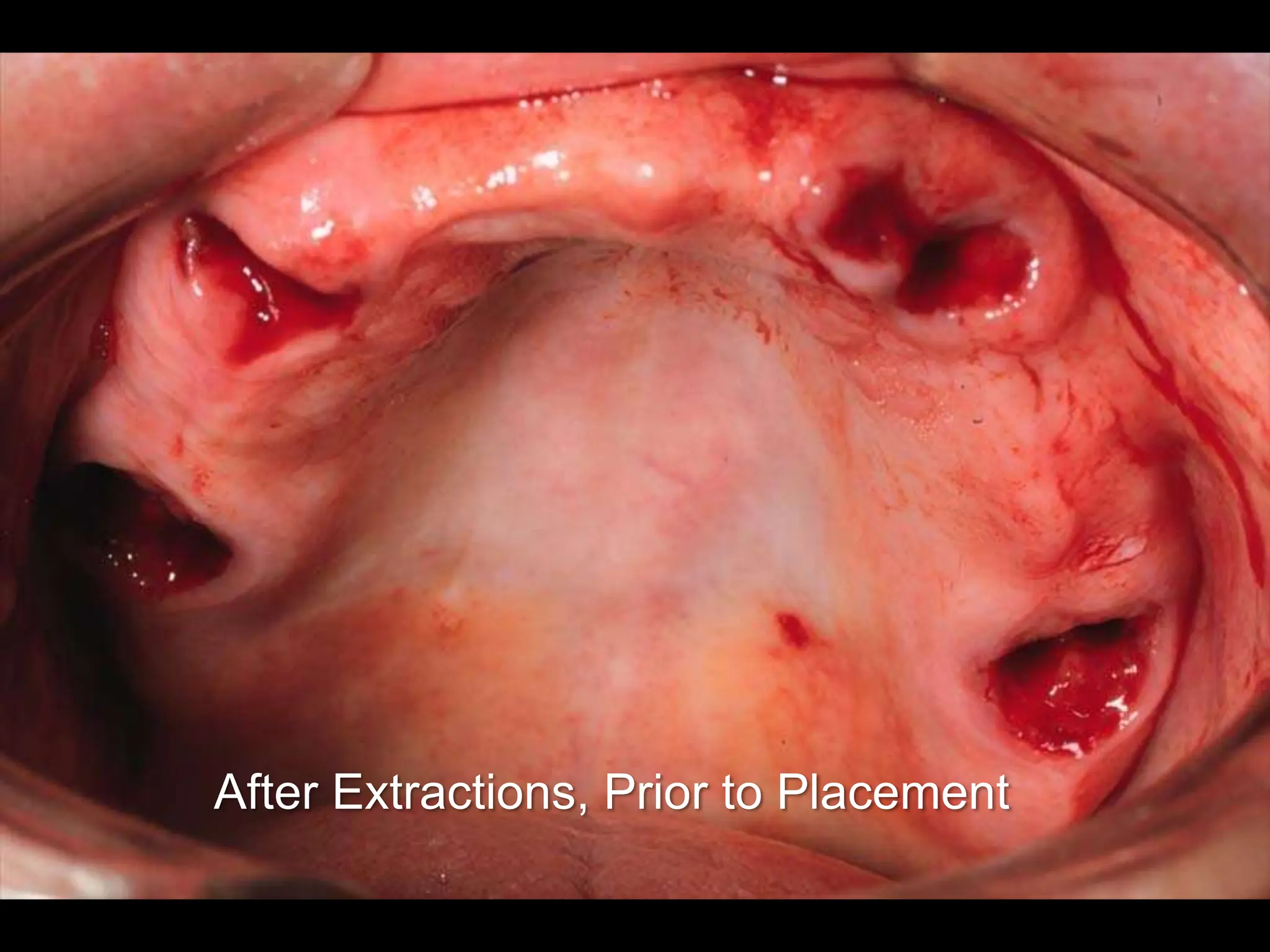
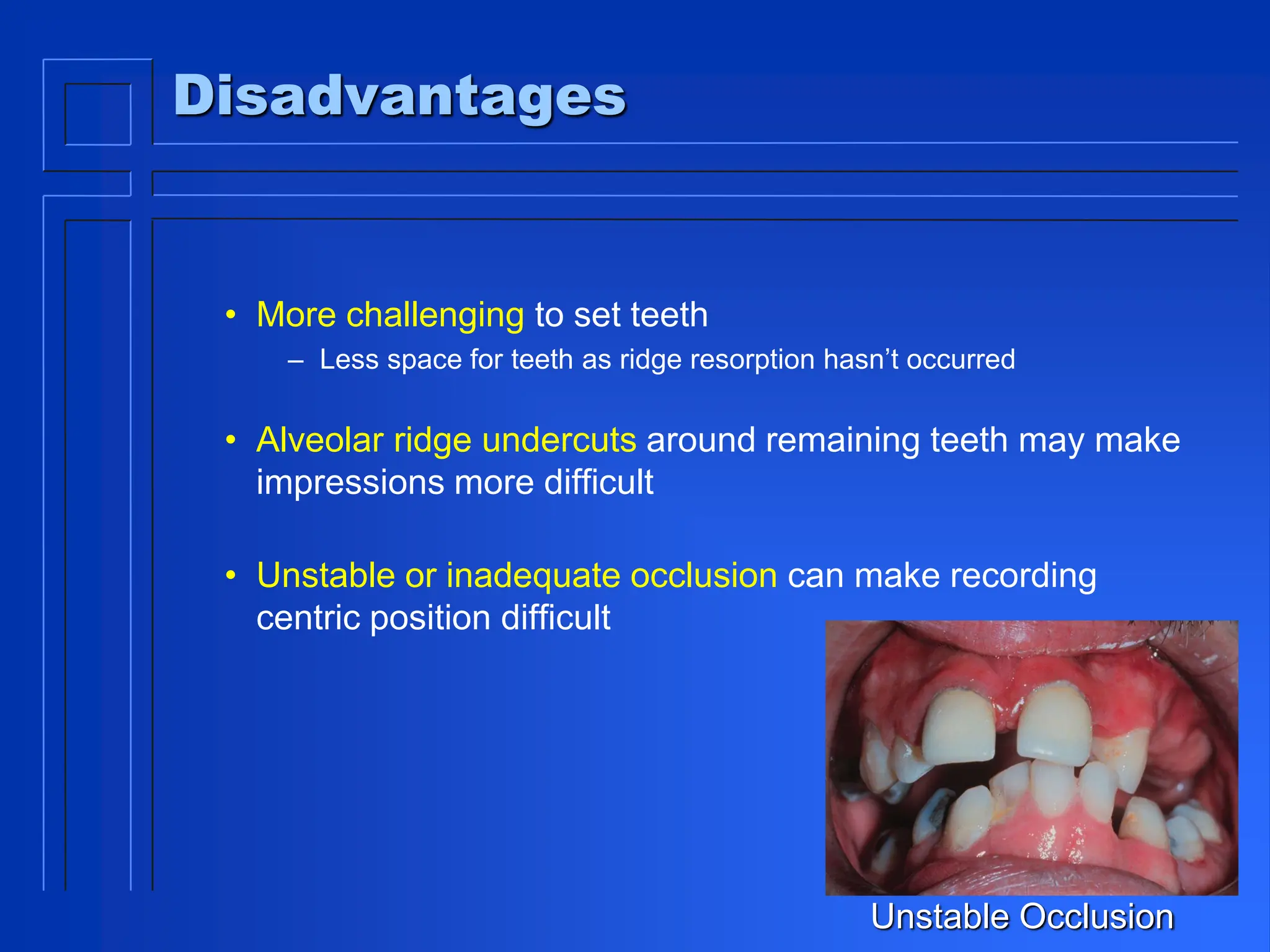
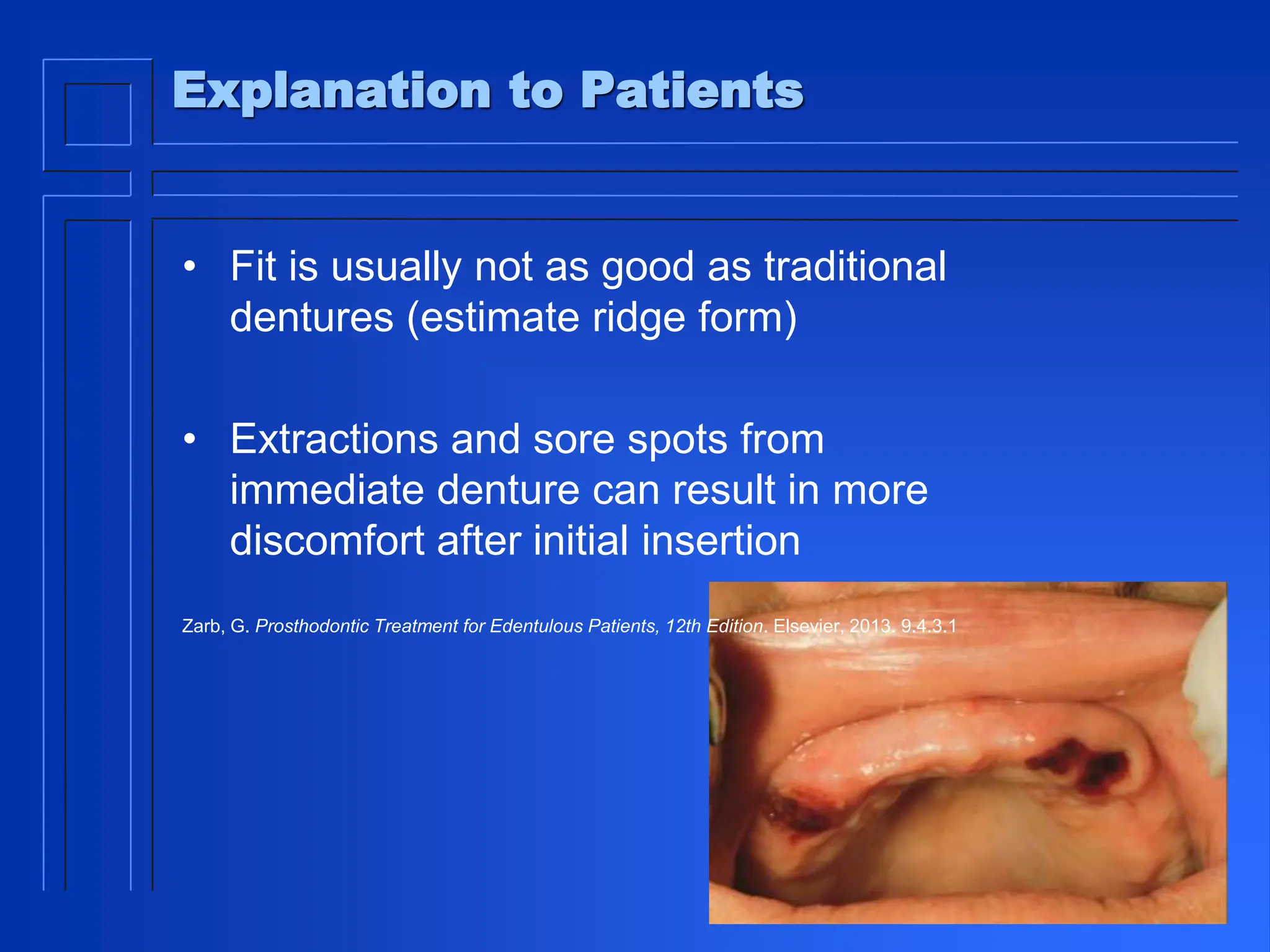
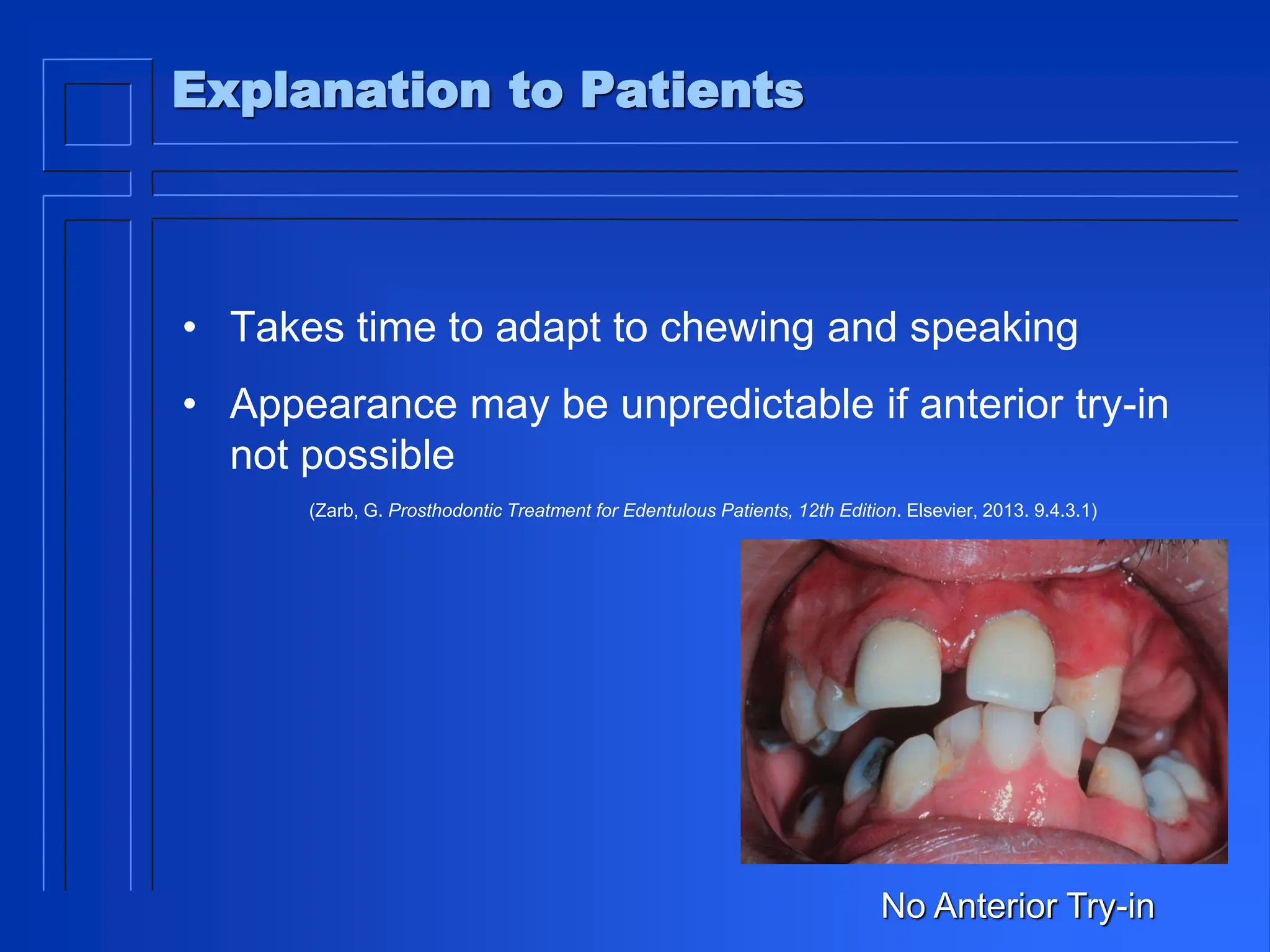
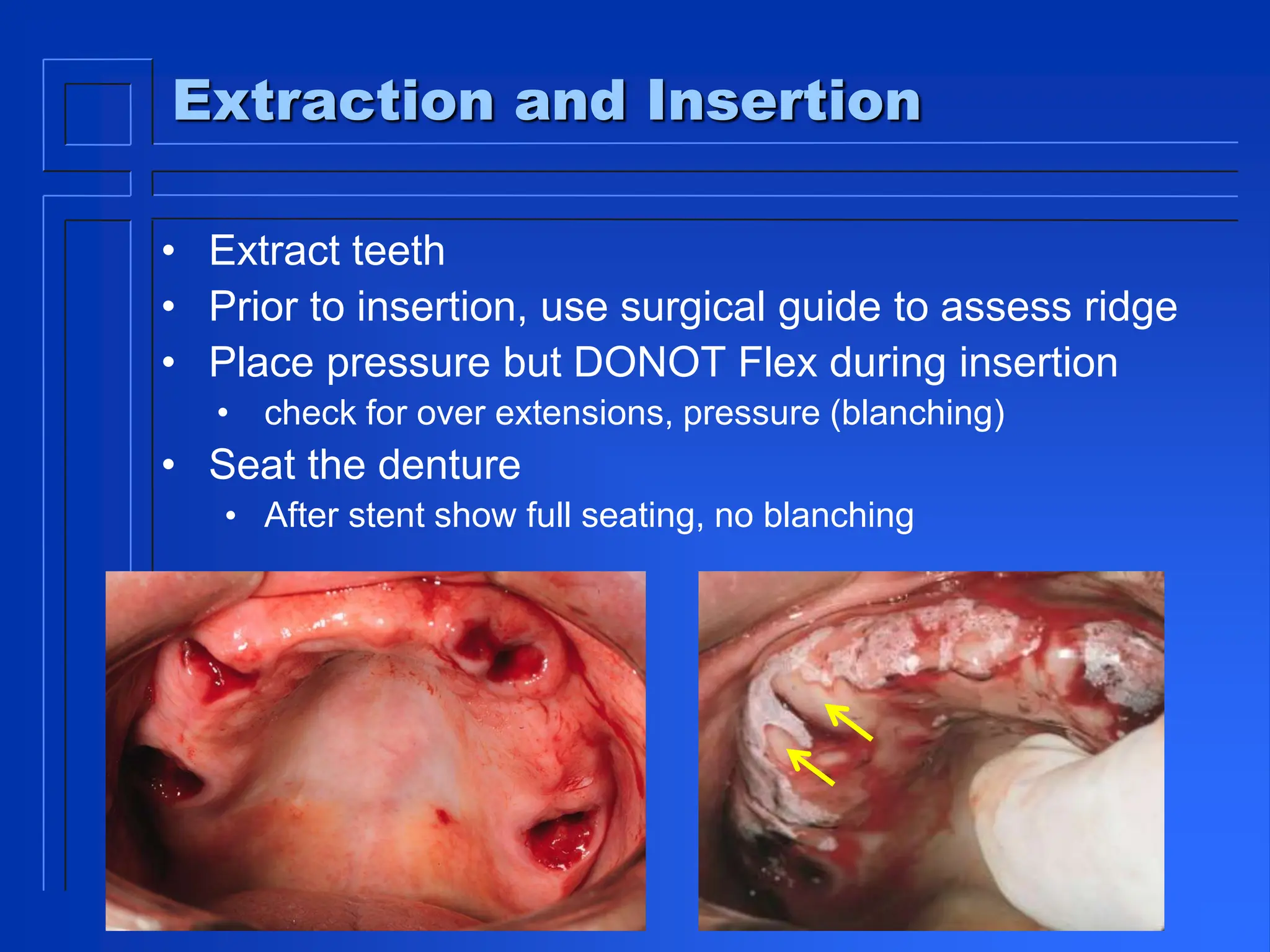
An immediate denture is a complete or partial denture fabricated and placed immediately following the extraction of natural teeth. It aims to maintain jaw relationships and support during healing. However, occlusion may be difficult to set due to limited tooth positioning and unstable ridges. The denture will require relines as the ridges resorb during healing. Patients are advised the fit will not be optimal initially and further adjustments may be needed. The denture should be inserted carefully following extractions and not removed for 24 hours to allow proper seating and healing. Follow up appointments in 1 week and 1 month allow for adjustments and improving retention as the ridges adapt.