Impacted lower and upper 3rd molar lecture
•Download as DOC, PDF•
14 likes•1,805 views

This document summarizes the surgical procedures and considerations for extracting impacted third molars. It describes the different types of impactions - mesioangular, vertical, horizontal, and distoangular - and the techniques for removing each, such as sectioning the tooth and removing bone. Potential complications are outlined, including bleeding, swelling, trismus, pain, infection, root fracture, and alveolar osteitis. Methods to prevent and treat complications are provided, such as the use of antibiotics, steroids, irrigation, and dressings. Surgical success depends on factors like impaction depth and the surgeon's experience.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Impacted lower and upper 3rd molar lecture
Similar to Impacted lower and upper 3rd molar lecture (20)
More from memoalawad
More from memoalawad (20)
Recently uploaded
Recently uploaded (20)
Impacted lower and upper 3rd molar lecture
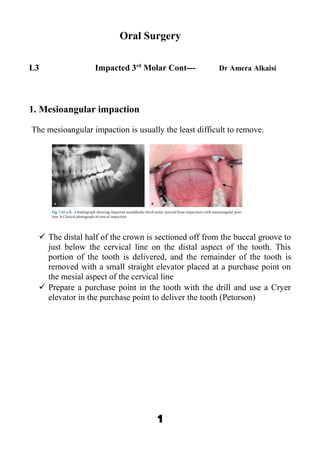
- 1. Oral Surgery L3 Impacted 3rd Molar Cont--- Dr Amera Alkaisi 1. Mesioangular impaction The mesioangular impaction is usually the least difficult to remove. The distal half of the crown is sectioned off from the buccal groove to just below the cervical line on the distal aspect of the tooth. This portion of the tooth is delivered, and the remainder of the tooth is removed with a small straight elevator placed at a purchase point on the mesial aspect of the cervical line Prepare a purchase point in the tooth with the drill and use a Cryer elevator in the purchase point to deliver the tooth (Petorson) 1
- 2. The bone covering the tooth is removed using a round bur, until the entire crown is exposed. Using a fissure bur, sufficient bone is removed using the guttering technique, on the buccal and mainly the distal aspect of the tooth. 2
- 3. If the tooth is single-rooted, to facilitate its removal, the mesial portion of the tooth is removed first, while the remaining portion is then luxated. If the tooth has two roots, the roots may be separated and each root may be extracted in the easiest direction, depending on its curvature. More specifically, a deep vertical groove is made on the crown of the tooth using a fissure bur, approximately as far as the intra radicular bone. Sectioning is achieved using a straight elevator, which, after being placed in the groove already created, is rotated and separates the 3
- 4. roots. This separation of the tooth allows for limited bone removal, thus causing less trauma and faster completion of the surgical procedure. 4
- 5. Bone removed buccaly & distally. The cut is increase to level of the bifurcation & the chisel used to section the distal half of the crown of the 5
- 6. third molar or to section vertically through its bifurcation. The distal crown segment or the distal crown segment & attached root are removed as a single unit. The mesial portion is tightly wedged under the second molar. The bur can be used to cut a deep groove in mesial root beginning in the pulp camper so an elevator can split the crown from the root then they removed separately. 2. Vertical impaction: The vertical impaction is one of the more difficult ones to remove, especially if it is deeply impacted. The procedure for bone removal and sectioning is similar to that for the mesioangular impaction in that occlusal, buccal, and judicious distal bone is removed first Bone removal usually by splitting technique using chisel & malate or by bur technique which preferable in patient locally anaesthetized. Point of application created mesially or buccaly then by straight elevator the tooth is delivered. Or the distal half of the crown is sectioned and removed, and the tooth is elevated by applying a small straight elevator at the mesial aspect of the cervical line. The option of preparing a purchase point in the tooth is also frequently used, as for the mesioangular impaction(Peterson) 3.Horizontal impaction 6
- 7. The tooth may be superficial or deep in the bone and frequently its crown is close to the distal aspect of the second molar. The horizontal impaction usually requires the removal of more bone than the mesioangular impaction. Tooth neck is exposed by bur technique and the crown separated from the root & removed with a Cryer elevator. The roots are then displaced into the socket that was previously occupied by the crown and delivered into the mouth. Occasionally, they may need to be sectioned into separate portions and delivered independently. A groove is then created vertically to the long axis of the tooth using a fissure bur, at the cervical line of the tooth, to separate the crown from the root The groove created by the bur should not be deep since the mandibular canal is often found in close proximity to the tooth and there is a risk of injuring or severing the inferior alveolar nerve. The straight elevator is used, after being placed in the groove created earlier, to separate the crown from the root with a rotational movement. The crown is removed using movement upwards, and the root is then easily removed. - 7
- 8. 8
- 9. 9
- 10. 10
- 11. 4. Distoangular The most difficult tooth to remove, since it is located beneath the anterior border of the ramus with a fair amount of bone above its crown while its roots are inclined somewhat near the distal root of the second molar. Therefore, it is impossible to remove the tooth in one piece, unless a large amount of bone is removed. After the distobuccal bone & buccal bone are removed, the crown is usually sectioned from the roots just above the cervical line and delivered with a Cryer elevator. A purchase point is then prepared in the tooth, and the roots are delivered. together or sectioned and delivered independently with a Cryer elevator (Prterson) or the distal portion of the tooth is sectioned or the tooth is divided through its bifurcation, or sectioning the tooth in half or section of crown from root, followed by separation of the mesial root distal root & removed separately 11
- 12. 12
- 13. Extraction of Impacted Third Molar in Edentulous Patient The surgical extraction of the third molar in edentulous patients is much easier and faster compared to dentulous patients. The second molar, the major problems faced in surgery of impacted mandibular third molars in dentulous patients which often hinders manipulations during the operation. is often missing; therefore, tooth sectioning is not necessary. Same principles are used. 13
- 14. Post extraction socket care (Socket toilet) • Débriding the wound of all particular bone chips and other debris. The best method is to mechanically débride the socket and the area under the flap with a periapical curette • A bone file should be used to smooth any rough sharp edges of the bone. • A mosquito hemostat is usually used carefully to remove any remnant of the dental follicle which is usually on the distal aspect of the second molar as well as bone fragments that may be present in the socket are removed. • The socket and wound should be thoroughly irrigated with saline or sterile water (30 to 50 mL is optimal).Within certain limitations, the more irrigation that is used, the less likely the patient is to have a dry socket, delayed healing, or other complications 14
- 15. Suturing After bleeding controlled the flap is sutured. The incision should usually be closed by primary intention. The flap is returned to its original position • Envelop flap requires a suture between buccal & lingual flaps distal to the second molar, the initial suture placed at the posterior aspect of the second molar continue to the posterior end of the incision • when the flap is extended to the papilla between the first & second molar both this & the sulcus incision need suturing to retain the flap in place (interdental papillae). After 7 days the suture is removed. Medications 1. Systemic Antibiotics Perioperative Systemic Antibiotics: prophylactic antibiotics are necessary in some surgical procedures. Surgery for the removal of impacted third molars clearly fits into the category of clean-contaminated surgery. The incidence of postoperative infections in a clean surgery is related more to operator technique than to the use of prophylactic antibiotic however, infection probably is a rare occurrence following third molar surgery. This means that it is unusual to see pain, swelling, and a production of purulence that requires incision and drainage or antibiotic therapy. The incidence of such infections is very low for most surgeons expect to have an infection rate in the range of 1 to 5% for all third molar procedures. it is unnecessary to use prophylactic antibiotics in third molar surgery to prevent postoperative infection in the normal healthy . A more subtle type of wound healing problem that occurs after the surgical removal of the impacted 15
- 16. mandibular third molar is alveolar ostitis or dry socket. This disturbance in wound healing is most likely caused by : • The combination of saliva and anaerobic bacteria. Techniques that reduce bacterial contamination of the socket The use of prophylactic antibiotics in third molar surgery, reduce the incidence of dry socket. Copious irrigation Preoperative rinses with chlorhexidine Placement of antibiotics in the extraction socket, are also effective. Although systemic antibiotics are effective in the reduction of postoperative dry socket, they are no more effective than are local measures. The increase of antibiotic-related complications, such as allergy, resistant bacteria, gastrointestinal side effects, and secondary infections, is not outweighed by the benefits. Therefore, the use of perioperative systemic antibiotic administration does not seem to be valid. Perioperative Steroids The use of corticosteroids to minimize swelling, trismus, and pain. The method of usage, is extremely variable, and the most effective therapeutic regimen has yet to be clearly delineated. • An initial intravenous dose of steroid at the time of surgery has a major clinical impact on swelling and trismus in the early postoper- ative period. • If the initial intravenous dose is not followed up with additional doses of steroids, this early advantage disappears by the second or third postoperative day. • Maximum control of swelling requires that additional steroids be given for 1 or 2 days following surgery. The two most widely used steroids are dexamethasone and methylprednisolone. Common dosages of dexamethasone are 4 to 12 mg IV at the time of surgery. Additional oral dosages of 4 to 8 mg bid on the day of surgery and for two days afterward result in the maximum relief of swelling, trismus, and pain. Methylprednisolone is most commonly given 125 mg IV at the 16
- 17. time of surgery followed by significantly lower doses, usually 40 mg PO tid or qid, later on the day of surgery and for two days after surgery. High-dose short-term steroid use is associated with minimal side effects. It is contraindicated in the patient with gastric ulcer disease, active infection, and certain types of psychosis. The administration of perioperative steroids may increase the incidence of alveolar osteitis after third molar surgery, but the data are lacking as to the precise degree of increase. Determinant of the incidence of complications of third molar surgery • The depth of impaction, that is, whether it is a complete bony impaction. The removal of complete bony impactions is likewise associated with increased postoperative pain and morbidity and an increase in the incidence of inferior alveolar nerve anesthesia. • The age of the patient. Removal of impacted teeth in the older patient is associated with a higher incidence of postoperative complications, especially alveolar osteitis, infections, mandible fracture, and inferior alveolar nerve anesthesia. • The relative experience and training of the surgeon. The less experienced surgeon will have a significantly higher incidence of complications than the trained experienced surgeon Complications: o Bleeding: can be minimized by using a good surgical technique and by avoiding the tearing of flaps or excessive trauma to the overlying soft tissue. The most effective way to achieve hemostasis following surgery is to apply a moist gauze pack directly over the site of the surgery with adequate pressure. application of topical thrombin on a small piece of absorbable gelatin sponge into the extraction socket. The socket can also be packed with oxidized cellulose o Swelling: Postsurgical edema or swelling is an expected sequel of third molar surgery. The parenteral administration of corticosteroids is frequently employed to help minimize the swelling that occurs. The application of ice packs to the face may make the patient feel more comfortable but has no effect on the magnitude of edema. The swelling usually reaches its peak by the end of the second postoperative day and is usually resolved by the fifth to 17
- 18. seventh day. This can be reduced by the use of the 10 mg of dexamethasone for 2 days o Trismus: is a normal and expected outcome following third molar surgery. Patients who are administered steroids for the control of edema also tend to have less trismus. Like edema, jaw stiffness usually reaches its peak on the second day and resolves by the end of the first week o Pain: it is normal consequence of surgery. The more extensive the surgery the more discomfort. The postsurgical pain begins when the effects of the local anesthesia subside and reaches its maximum intensity during the first 12 hours postoperatively. The most common analgesics are combinations of acetylsalicylic acid or acetaminophen with codeine, and the non steroidal anti inflammatory analgesics. Analgesics should be given before the effect of the local anesthesia subsides. The administration of nonsteroidal analgesics before surgery may be beneficial in aiding in the control of postoperative pain. The most important determinant of the amount of postoperative pain that occurs is the length of the operation. o Infection: Infection after removal of mandibular third molars is almost always a minor complication. About 50% of infections are localized subperiosteal abscess-type infections, which occur 2 to 4 weeks after a previously uneventful postoperative course. These are usually attributed to debris that is left under the mucoperiosteal flap and are easily treated by surgical débridement and drainage o Fracture of a portion of the root One of the most frequent problems encountered in removing third molars is the fracture of a portion of the root, which may be difficult to retrieve. In these situations the root fragment may be displaced into the submandibular space, the inferior alveolar canal, or the maxillary sinus. Uninfected roots left within the alveolar bone have been shown to remain in place without postoperative complications. The pulpal tissues undergo fibrosis, and the root becomes totally incorporated within the alveolar bone. Aggressive and destructive attempts to remove portions of roots that are in precarious positions seem to be unwarranted and may cause more damage than benefit. Radiographic follow-up may be all that is required 18
- 19. o Aveolar Osteitis The incidence of alveolar osteitis or dry socket following the removal of impacted mandibular third molars varies between 3 and 25%.The pathogenesis of alveolar osteitis has not been clearly defined, but the condition is most likely the result of lysis of a fully formed blood clot before the clot is replaced with granulation tissue. This fibrinolysis occurs during the third and fourth days and results in symptoms of pain and malodor after the third day or so following extraction. The source of the fibrinolytic agents may be tissue, saliva, or bacteria.The role of bacteria in this process can be confirmed empirically based on the fact that systemic and topical antibiotic prophylaxis reduces the incidence of dry socket by approximately 50 to 75%. The periodontal ligament may also play a role in the development of alveolar osteitis. The incidence of dry socket seems to be higher in patients who smoke in female patients who take oral contraceptives. Its occurrence can be reduced by several techniques, most of which are aimed at reducing the bacterial contamination of the surgical site. • Presurgical irrigation with antimicrobial agents such as chlorhexidine reduces the incidence of dry socket by up to 50%. • Copious irrigation of the surgical site with large volumes of saline is also effective in reducing dry socket. • Topical placement of small amounts of antibiotics such as tetracycline or lincomycin may also decrease the incidence of alveolar osteitis. Treatment The goal of treatment of dry socket is to relieve the patient’s pain during the delayed healing process. This is usually accomplished by irrigation of the involved socket, gentle mechanical débridement, and placement of an obtundent dressing, which usually contains eugenol. The dressing may need to be changed on a daily basis for several days and then less frequently after that. The pain syndrome usually resolves within 3 to 5 days, although it may take as long as 10 to 14 days in some patients. There is some evidence that topical antibiotics such as metronidazole may hasten resolution of the dry socket. In summary, alveolar osteitis is a disturbance in healing that occurs after the formation of a mature blood clot but before the blood clot is replaced with 19
- 20. granulation tissue. The primary etiology appears to be one of excess fibrinolysis, with bacteria playing an important but yet ill-defined role. Antimicrobial agents delivered by perioperative mouth rinses, topical- ly placed in the socket, or administered systemically all help to reduce the incidence of dry socket. Mechanical débridement and copious saline irrigation of the surgical wound also are effective in reducing the incidence of dry socket. A rational approach may be to provide preoperative chlorhexidine rinses for approximately 1 week before surgery, irrigate the wound thoroughly with normal saline at the conclusion of surgery, place a small square of gelatin sponge saturated with tetracycline in the socket, and continue chlorhexidine rinses for 1 additional week. This combination approach should substantially reduce the incidence of dry socket. o Nerve Disturbances: Surgical removal of mandibular third molars places both the lingual and inferior alveolar branches of the third division of the trigeminal nerve at risk for injury. The incidence of injury to the inferior alveolar and lingual nerves following third molar surgery is about 3%, Only a small proportion of these anesthesia and paresthesia problems remain permanent The lingual nerve is most often injured during soft tissue flap reflection Inferior alveolar nerve is injured when the roots of the teeth are manipulated and elevated from the socket. Mostly occur in complete bony impaction of mandibular third molars. The angulation classifications most commonly involved are usually mesioangular and vertical impaction. In some cases, nerve proximity to the root is indicated by an apparent narrowing of the inferior alveolar canal as it crosses the root or severe root dilaceration adjacent to the canal. diversion of the path of the canal by the tooth, darkening of the apical end of the root indicating that it is included within the canal, and interruption of the radiopaque white line of the canal. o Periodontal pocketing down the distal aspect of the second molar is late complication. If the third molar is partially impacted and is partially exposed in the mouth, it should be removed as soon as possible. The reason for this is that there is already a deep and potentially destructive periodontal lesion that is difficult for the patient to maintain hygienically. Even if the patient is asymptomatic, the impacted tooth should be removed as soon as 20
- 21. possible to allow the best periodontal healing after surgery as possible. In these situations the periodontal healing is compromised because of the fact that there was already a destructive lesion caused by the presence of the partially impacted third molar o Fracture of the mandible. Rarely occur. L4 O.Surgery Dr Amera Alkaisi Maxillary third molars 21
- 22. Surgical technique Incision: The most commonly used incision used for the maxillary third molar is also an envelope incision. It extends posteriorly from the 22
- 23. distobuccal line angle of the second molar and anteriorly to the first molar. A releasing incision is rarely necessary for the maxillary third molar.An incision is made diagonally across the tuberosity from its distopalatal aspect to distobuccal corner of the second molar & on in almost the same line up into buccal sulcus. If we need more bone removal the incision is extended around the upper second molar to its mesial aspect & mesial papilla included before its taken into the sulcus. Bone removal For maxillary teeth, bone removal is done primarily on the lateral aspect of the tooth down to the cervical line to expose the entire clinical crown. Frequently, the bone on the buccal aspect is thin enough that it can be removed with a periosteal elevator or a chisel using manual digital pressure. Maxillary verticle impaction: -The thin bone overlying the buccal surface of the tooth is removed. Bur is introduced back of the distal surface to create space for backward movement. A thin 23
- 24. bladed instrument (straight elevator ) is introduced between teeth, if we can’t introduce the instrument a hole is drilled into the buccal surface of the impaction to allow purchase by sharp elevator to move the tooth downward & backward. A straight Warwick James elevator used & placed mesial to the neck of third molar. 1. Maxillary mesioangular: Bone removal around the impacted tooth small currate to be sure if there is space between third molar & second molar acurved Warwick James elevator can be used to remove the tooth. 2. Maxillary distoangular: Buccal & alveolar bone is removed. The area distal to the impaction is carefully exposed. The tooth is elevated from the purchase on mesial side. The tooth can be pushed into antrum or into the tissue back of tuberocity. 24
- 25. Complications: Excessive bleeding from the sulcus incision. Haematoma formation with periorbital edema. Oro-antral fistula arise after elevation, but it heals if wound is suture. Displacement of wisdom tooth into antrum will require removal through a Caldwell-Luc antrostomy. 25
- 26. Occasionally the tooth displaced into infratemporal fossa lateral to ptrygoid plates. Fracture of the tuberosity espicially when the tooth roots are hypercementosed. 26