Download as PDF, PPTX






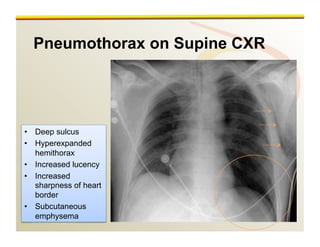


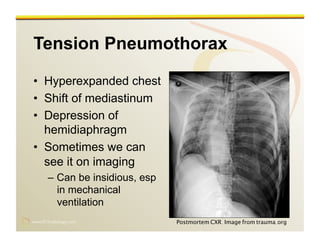
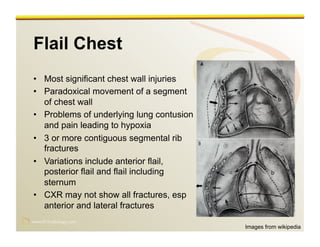





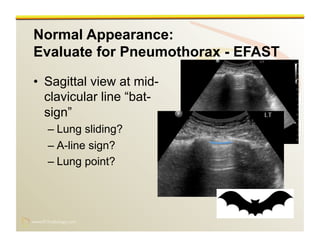




















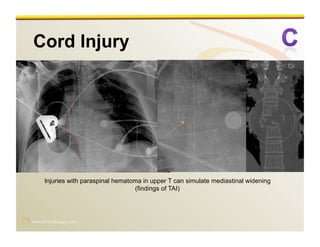











This document provides an overview of imaging techniques used in the evaluation of thoracic trauma. It begins with an introduction to the epidemiology of thoracic injuries and the importance of rapid diagnosis. The initial assessment involves a primary and secondary survey with a focus on airway, breathing and circulation. The imaging survey typically begins with a portable chest x-ray to evaluate for pneumothorax, hemothorax and other injuries followed by an ultrasound to assess for pericardial effusion. Additional sections discuss specific injuries like flail chest, hemothorax and tension pneumothorax that may be seen on CXR. The role of CT in thoracic trauma evaluation is also reviewed.






























































![Radiological_diagnosis_of_TB_ECHO_MOH[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicaldiagnosisoftbechomoh1-240905083452-eb26e5f9-thumbnail.jpg?width=640&height=640&fit=bounds)











































