Downloaded 332 times







































































Imaging plays an important role in head and neck cancer by aiding in diagnosis, staging, treatment planning, response evaluation, and detecting recurrence. Common imaging modalities used include panoramic x-ray, x-ray of the paranasal sinuses, ultrasound of the neck, CT, MRI, and PET-CT. Each modality has advantages and limitations for evaluating the oral cavity, neck lymph nodes, and distant metastases. CT is often the initial study due to its wide availability and ability to detect bone invasion and lymph node metastases. MRI provides better soft tissue contrast for evaluating nerve and muscle involvement. PET-CT can detect occult primary tumors and distant metastases.
Introduction to imaging's importance in diagnosing, staging, treatment planning, and monitoring head and neck cancers.
Overview of various imaging modalities for head and neck evaluation: X-ray, Ultrasound, CECT, MRI, PET-CT.
Details on the indications for panoramic X-rays in oral cavity assessment, particularly for cancer diagnosis.
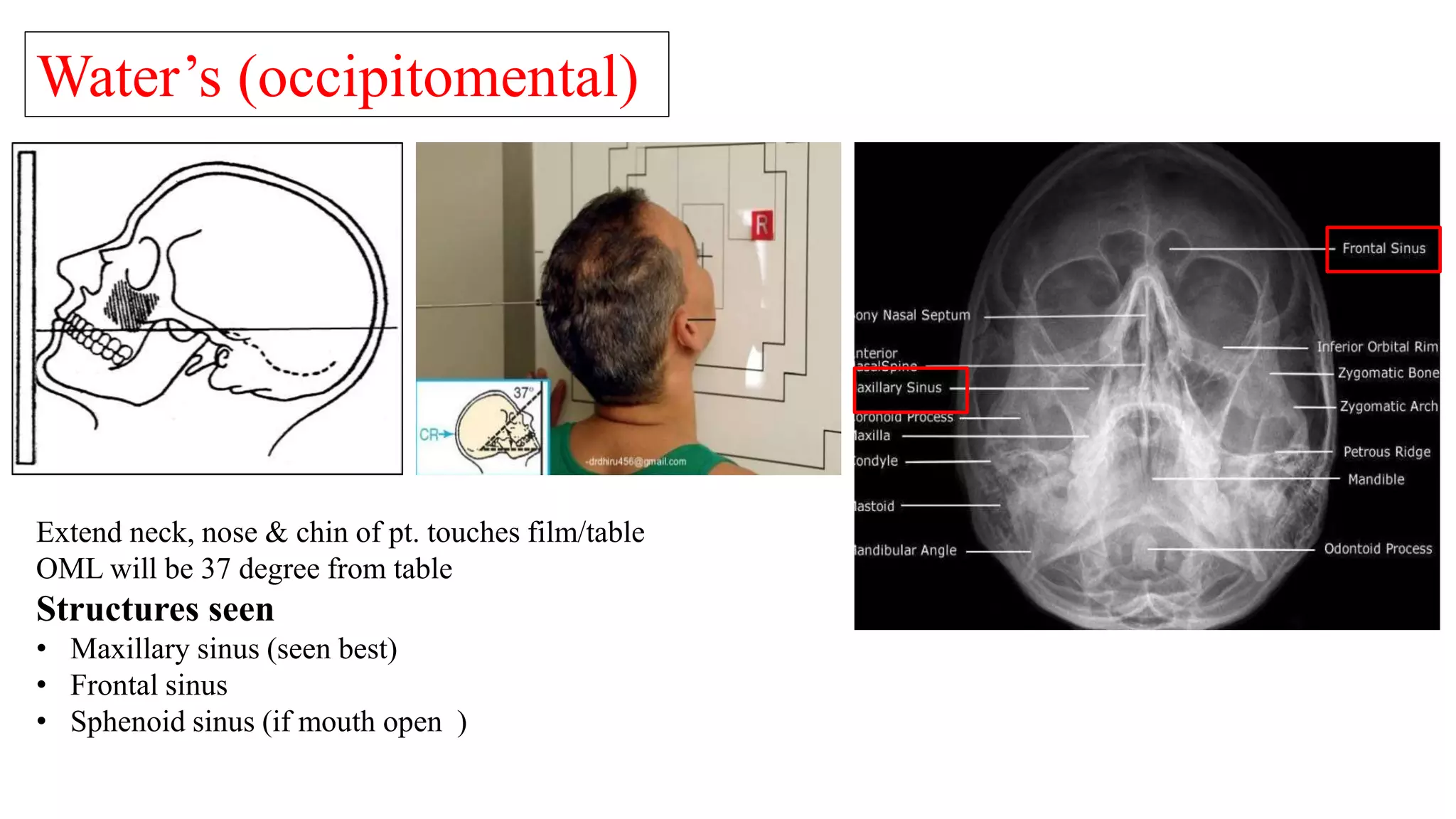
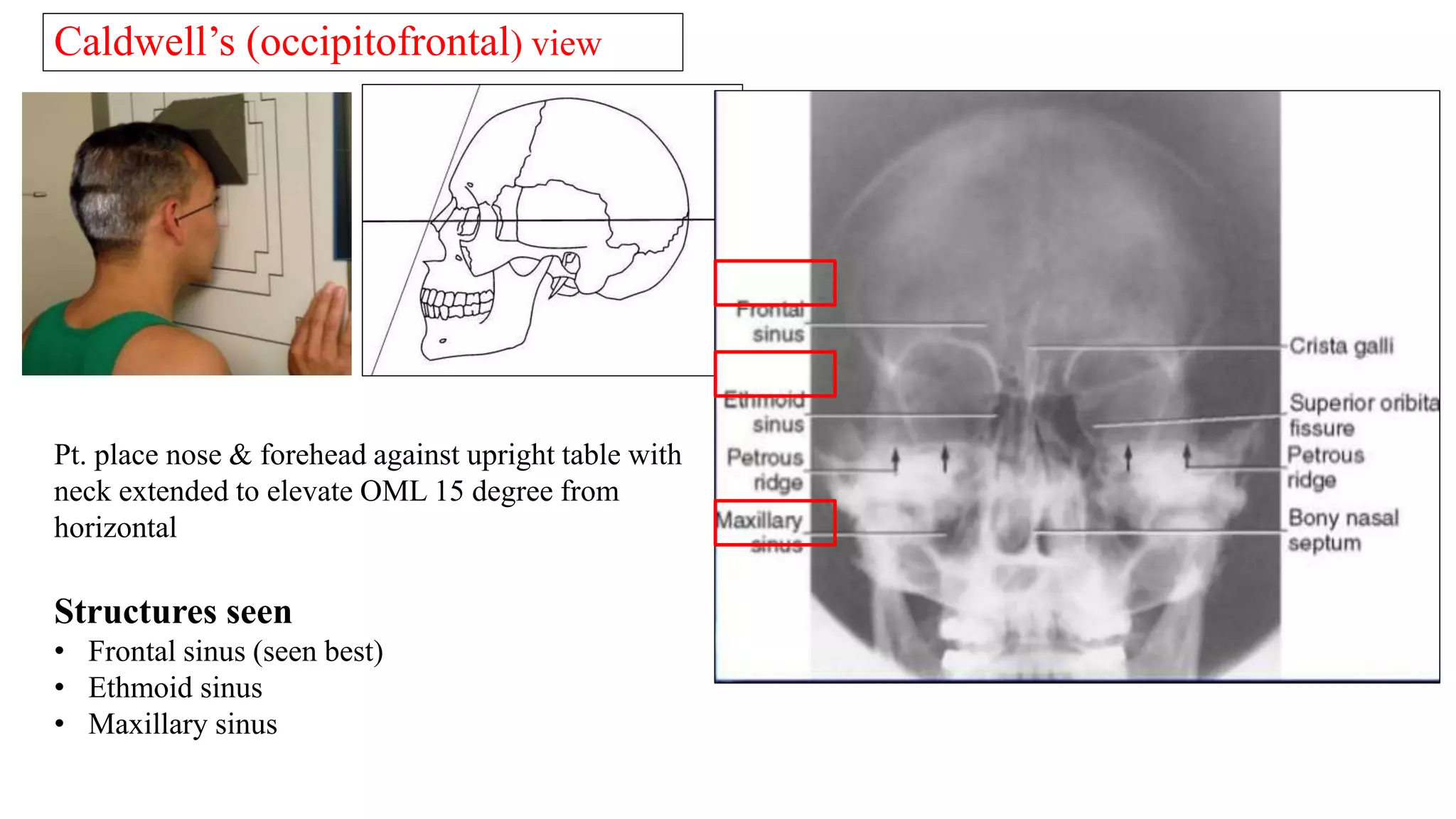
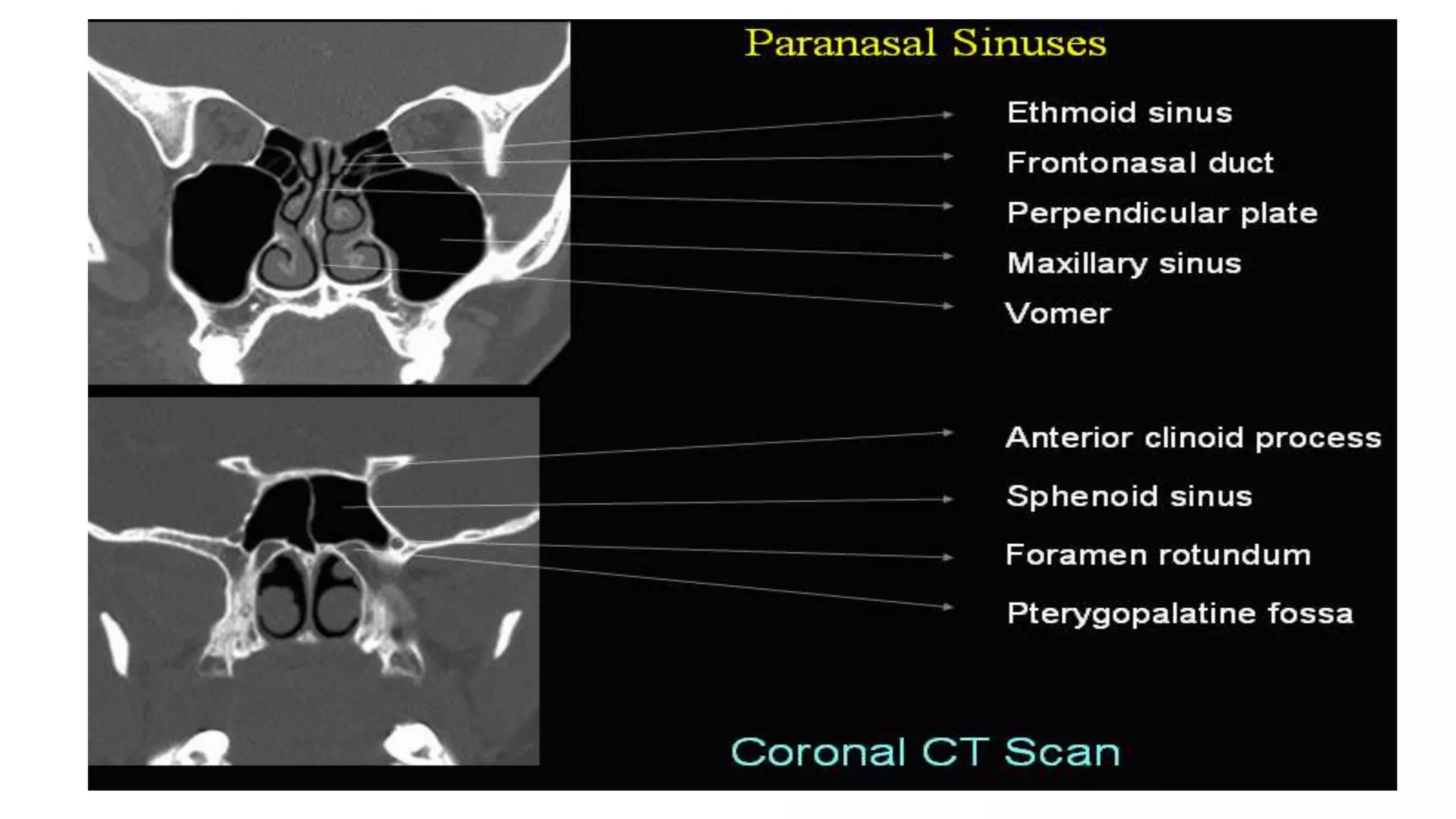
Description of paranasal sinus X-ray views, structures assessed, and pathological changes observed.
Utility of lateral soft tissue neck X-ray in identifying potential upper aerodigestive tract pathologies.
Benefits and limitations of ultrasound imaging for superficial lesions, lymph node assessment, and thyroid evaluation.
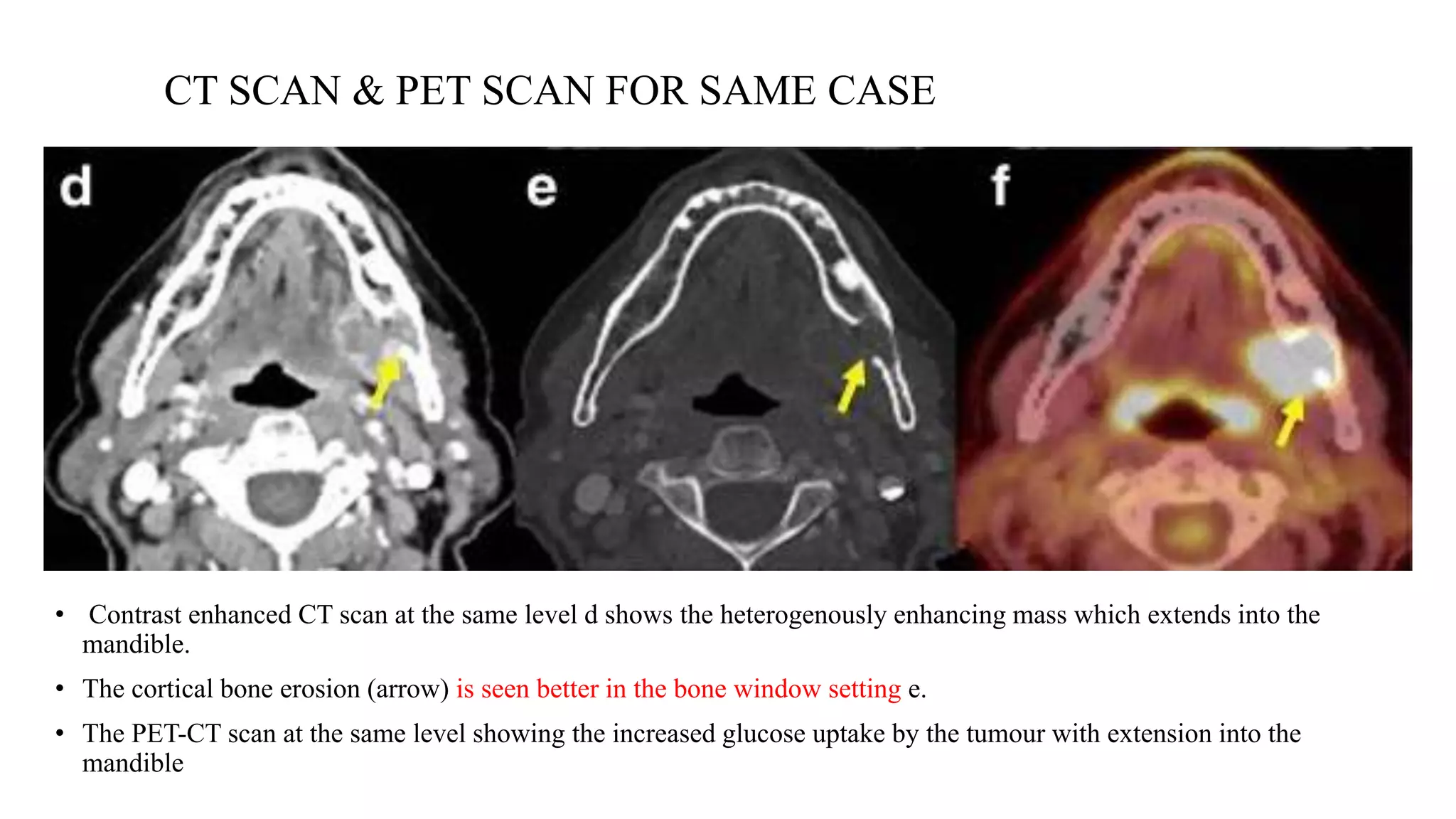
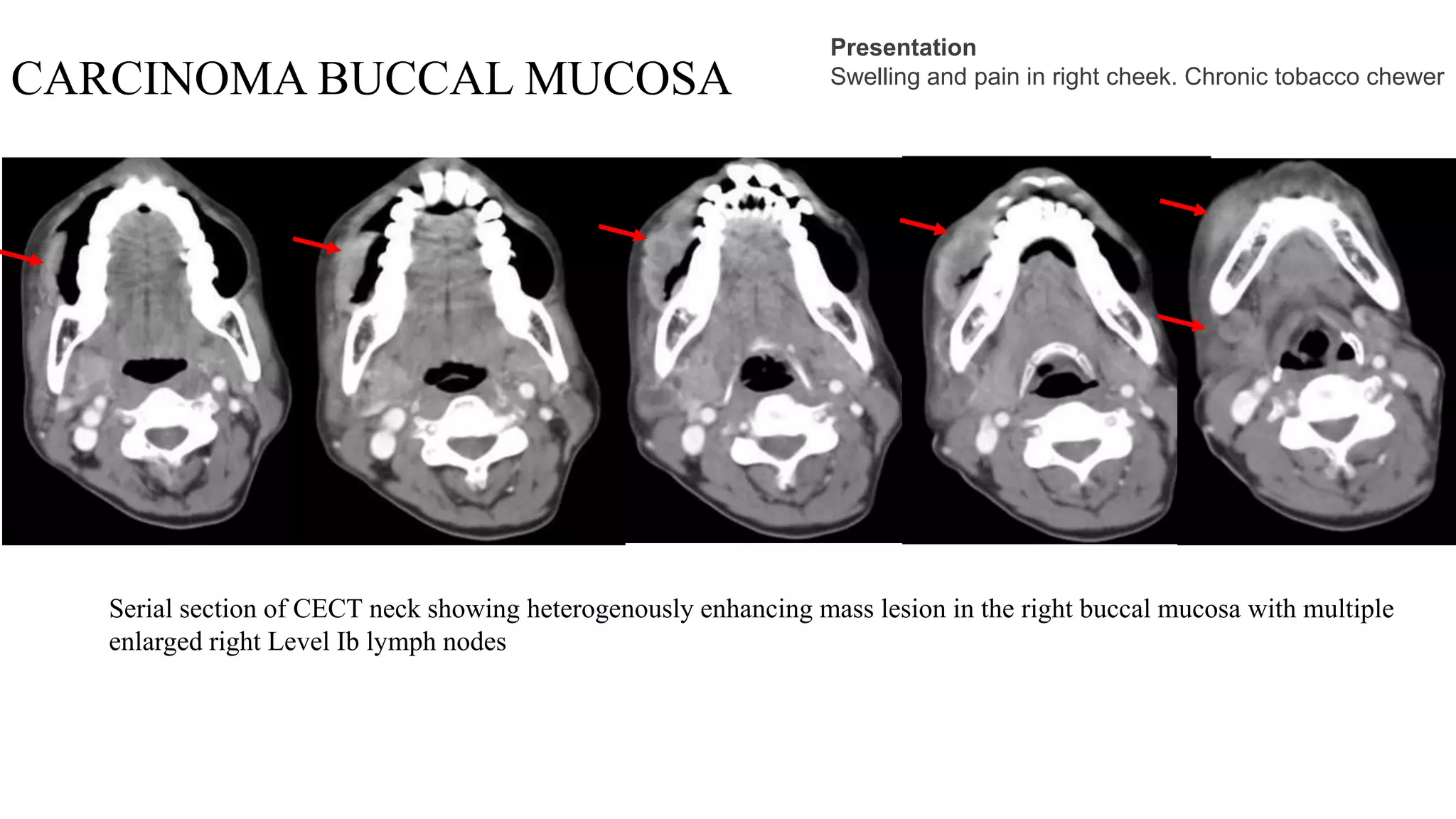
Importance of CECT scans in diagnosing malignancies, with key imaging features of tumors and lymph nodes.
MRI advantages in assessing malignancies, including tumor characteristics and differentiating from normal structures.
Functional imaging role of 18-FDG PET-CT in detecting tumors and evaluating metastatic disease and response.
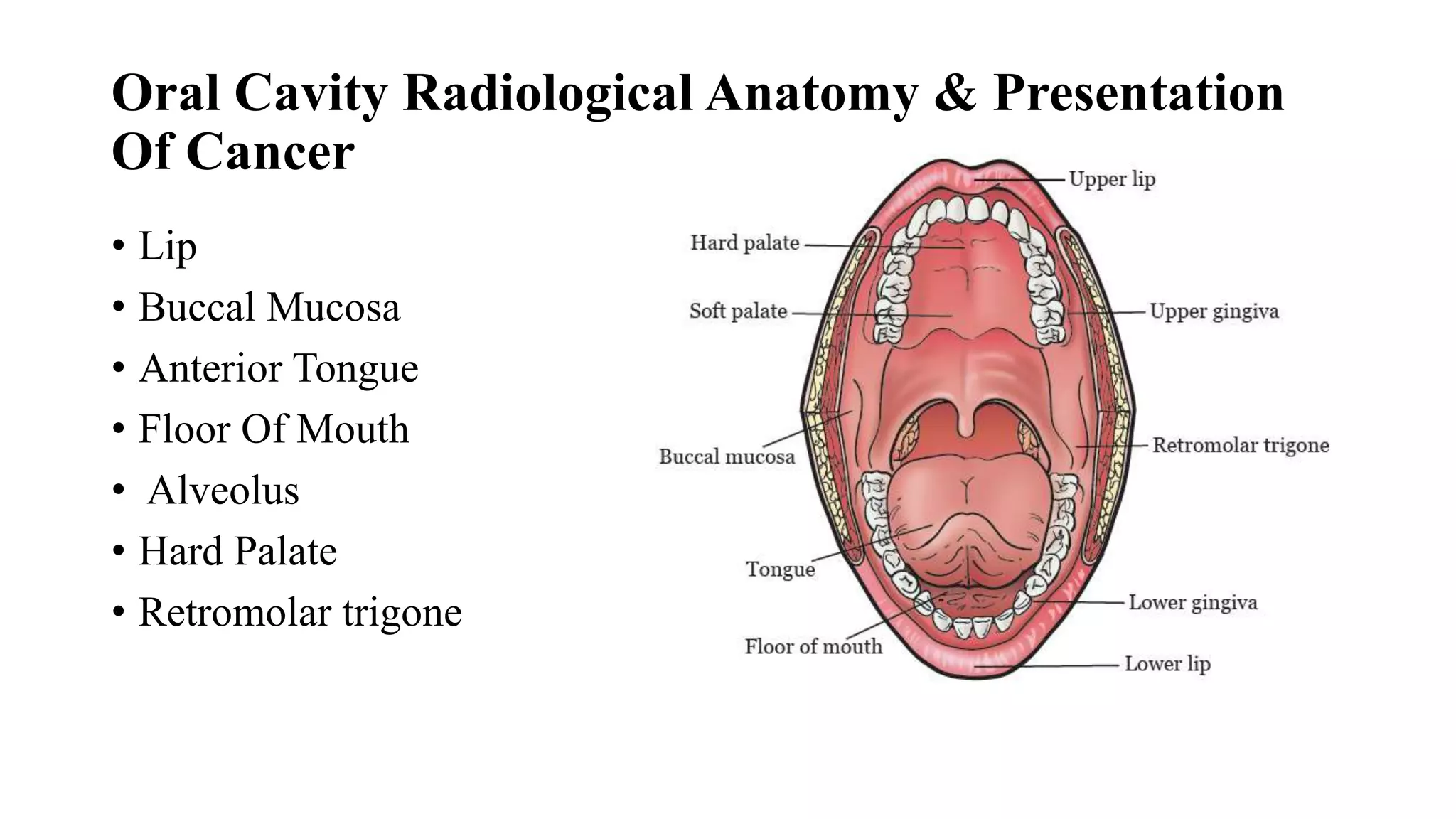
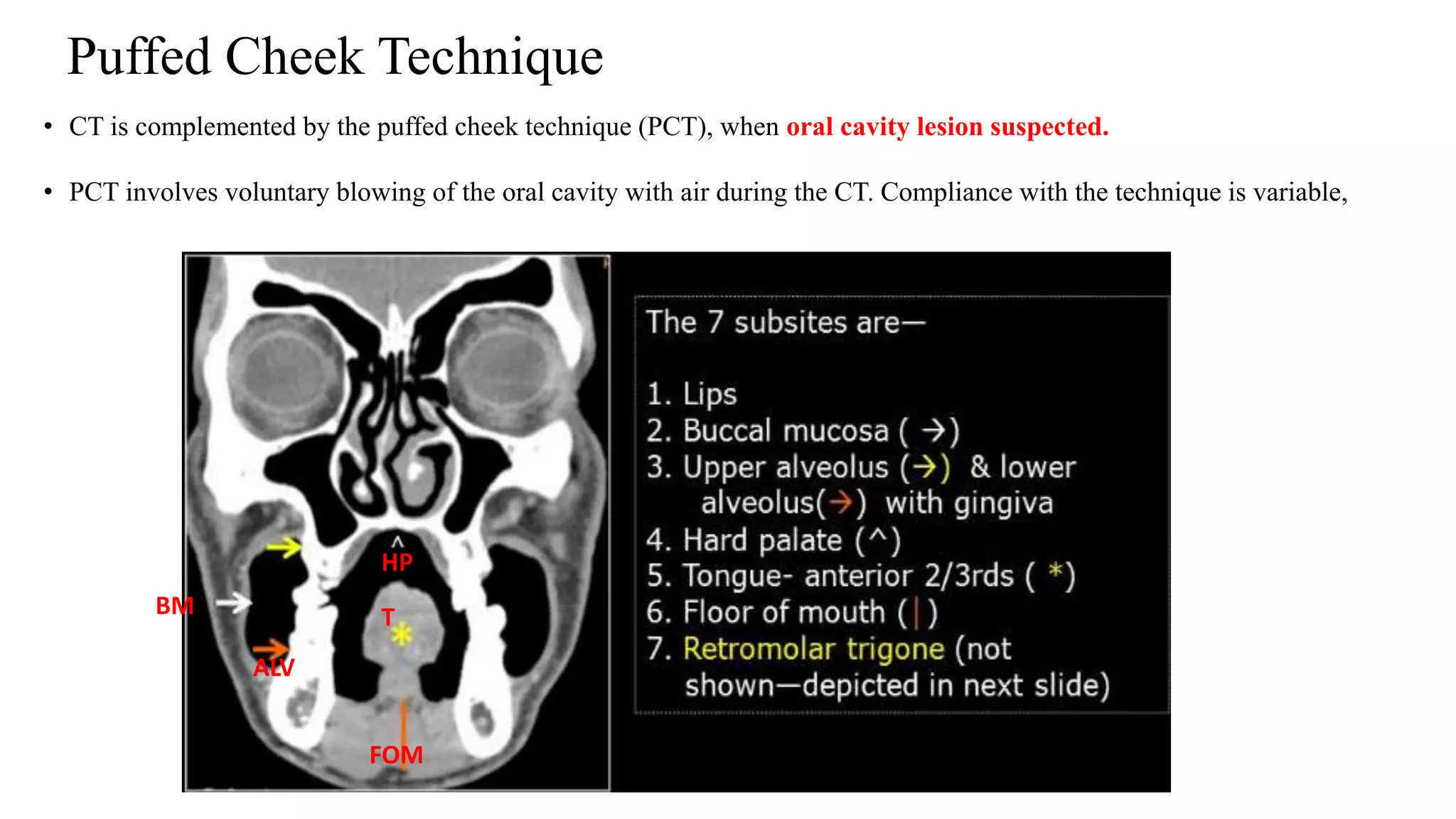
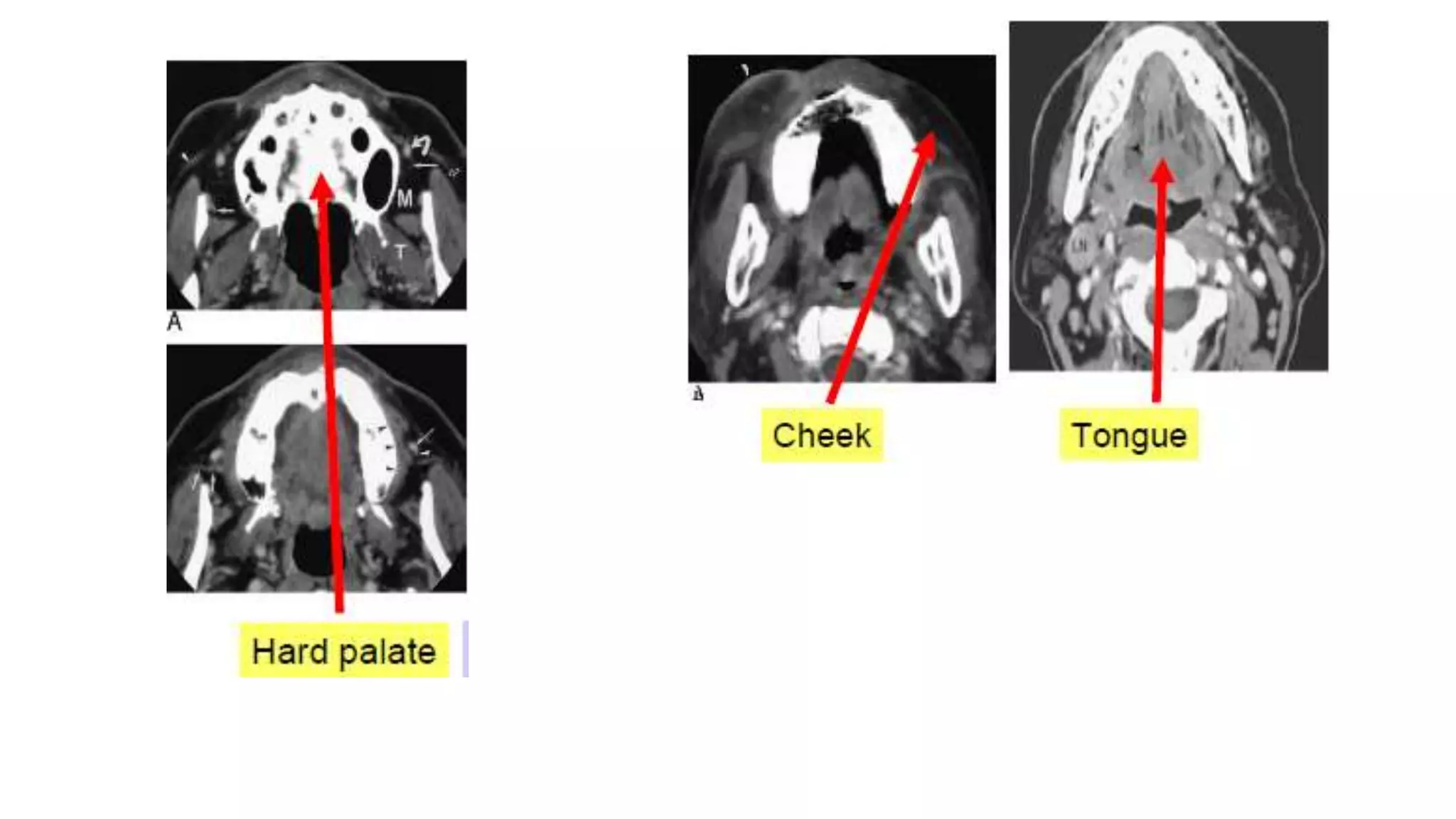
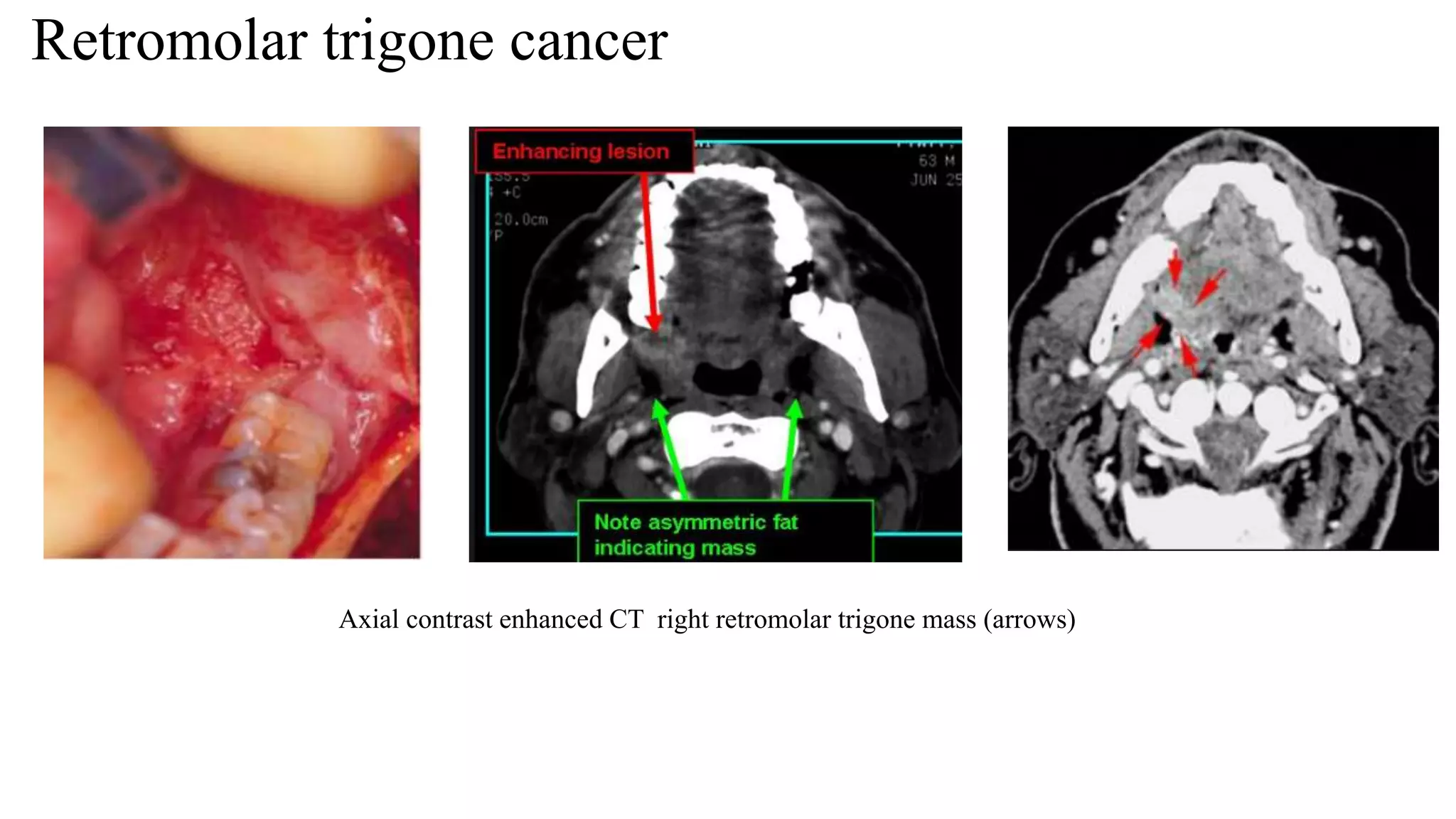
Anatomical overview of oral cavity regions affected by cancer, highlighting imaging techniques applied.
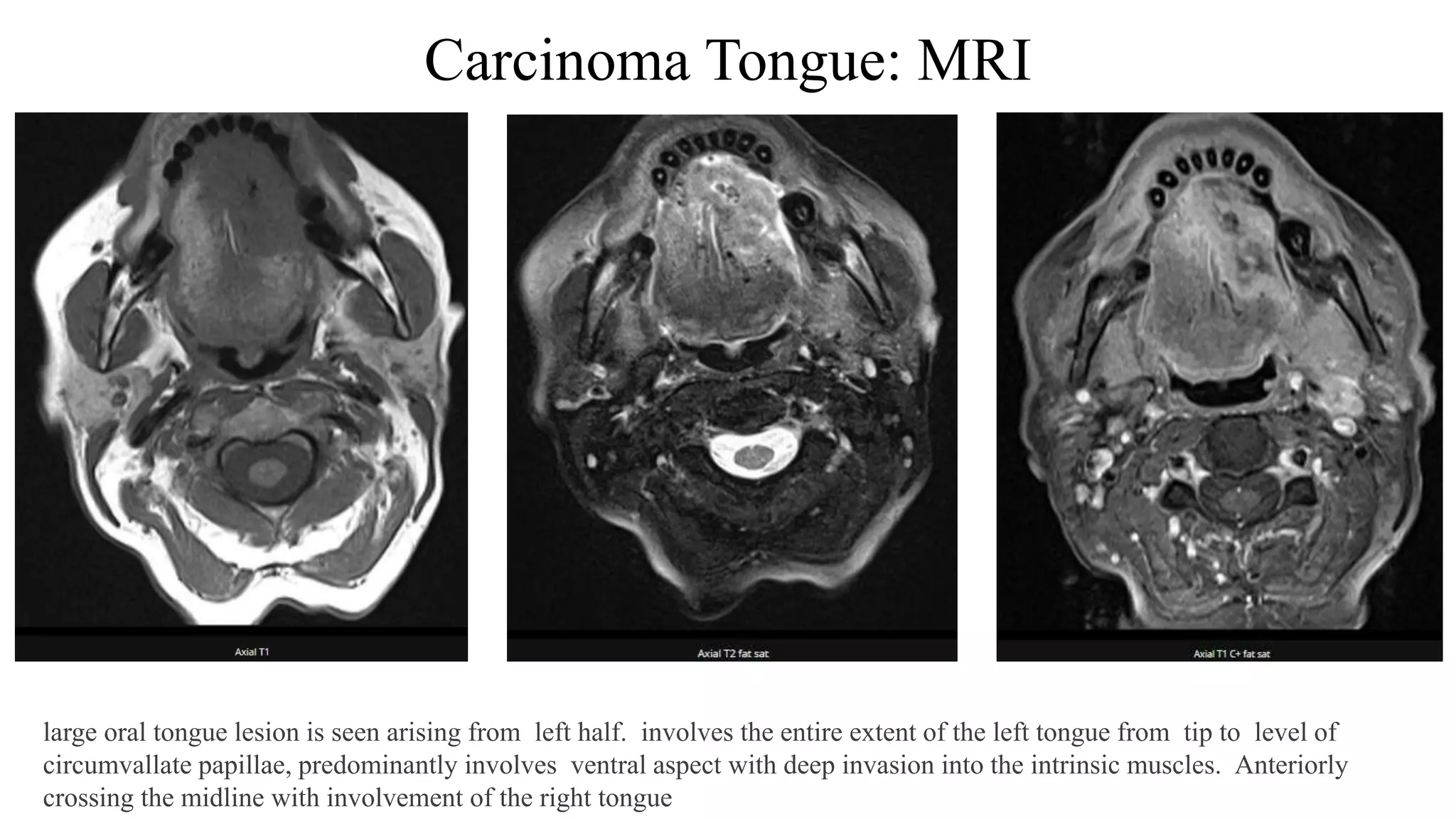
Clinical presentations and imaging characteristics of various oral cavity cancers such as tongue and buccal mucosa.
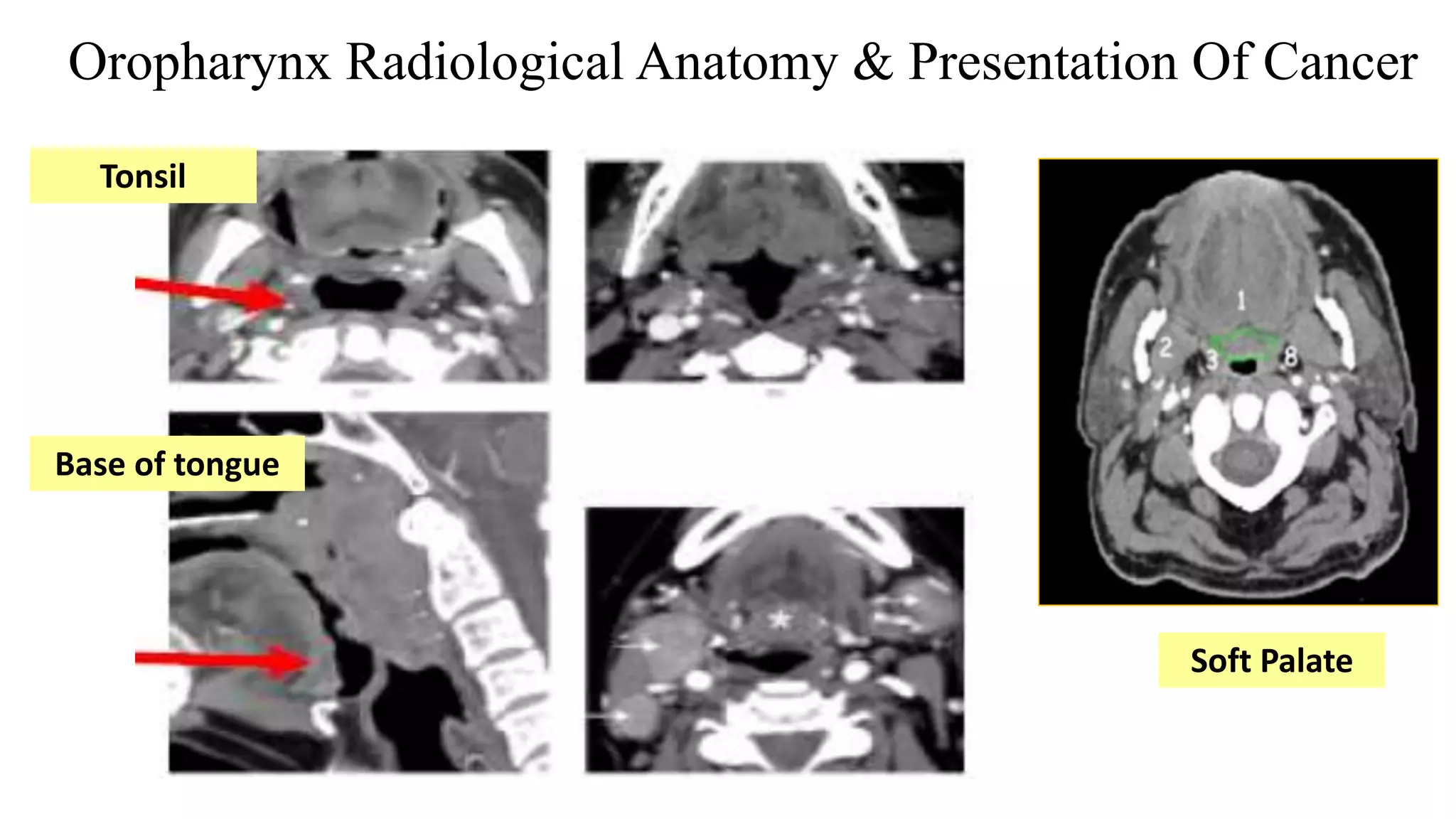
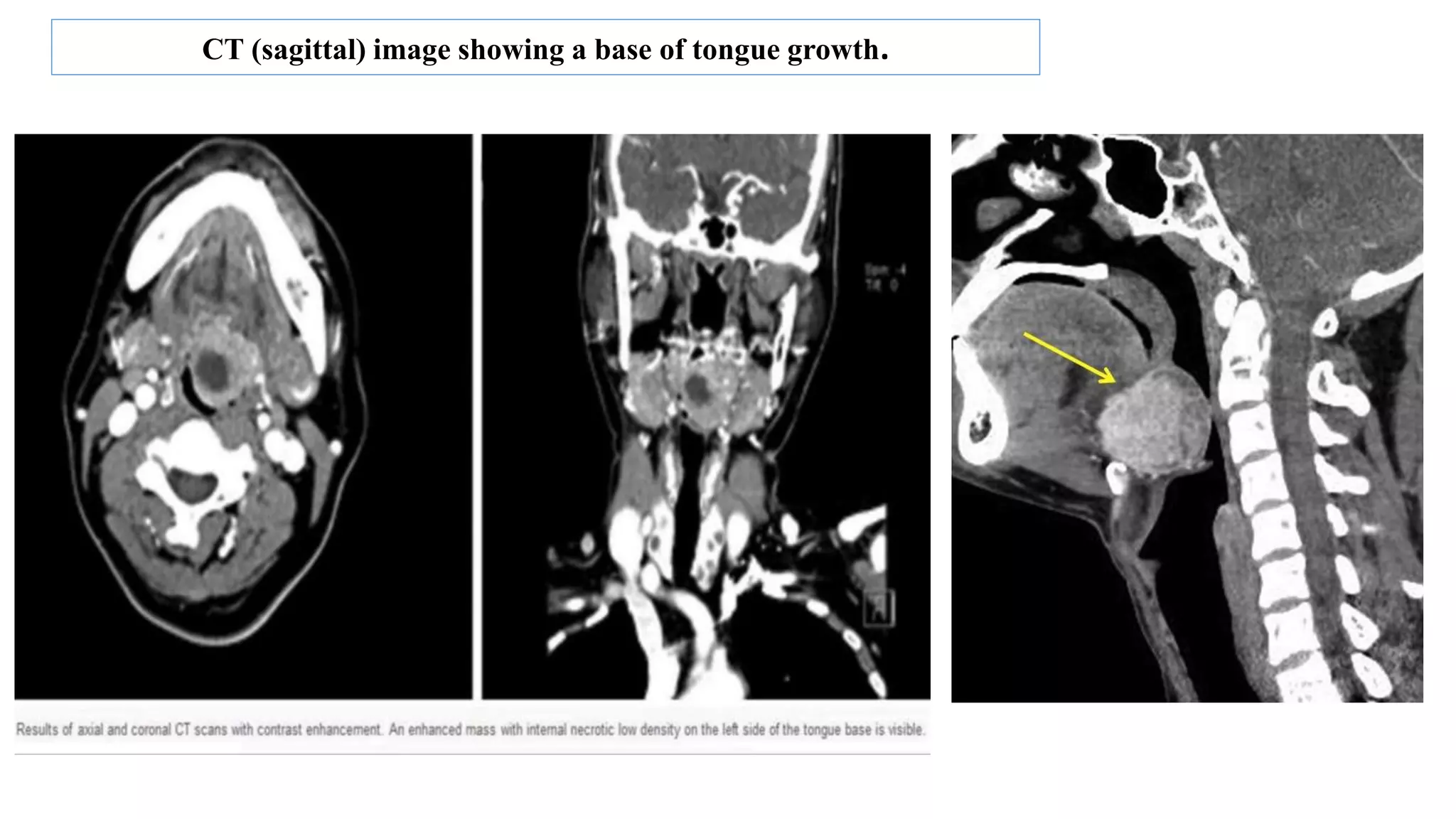
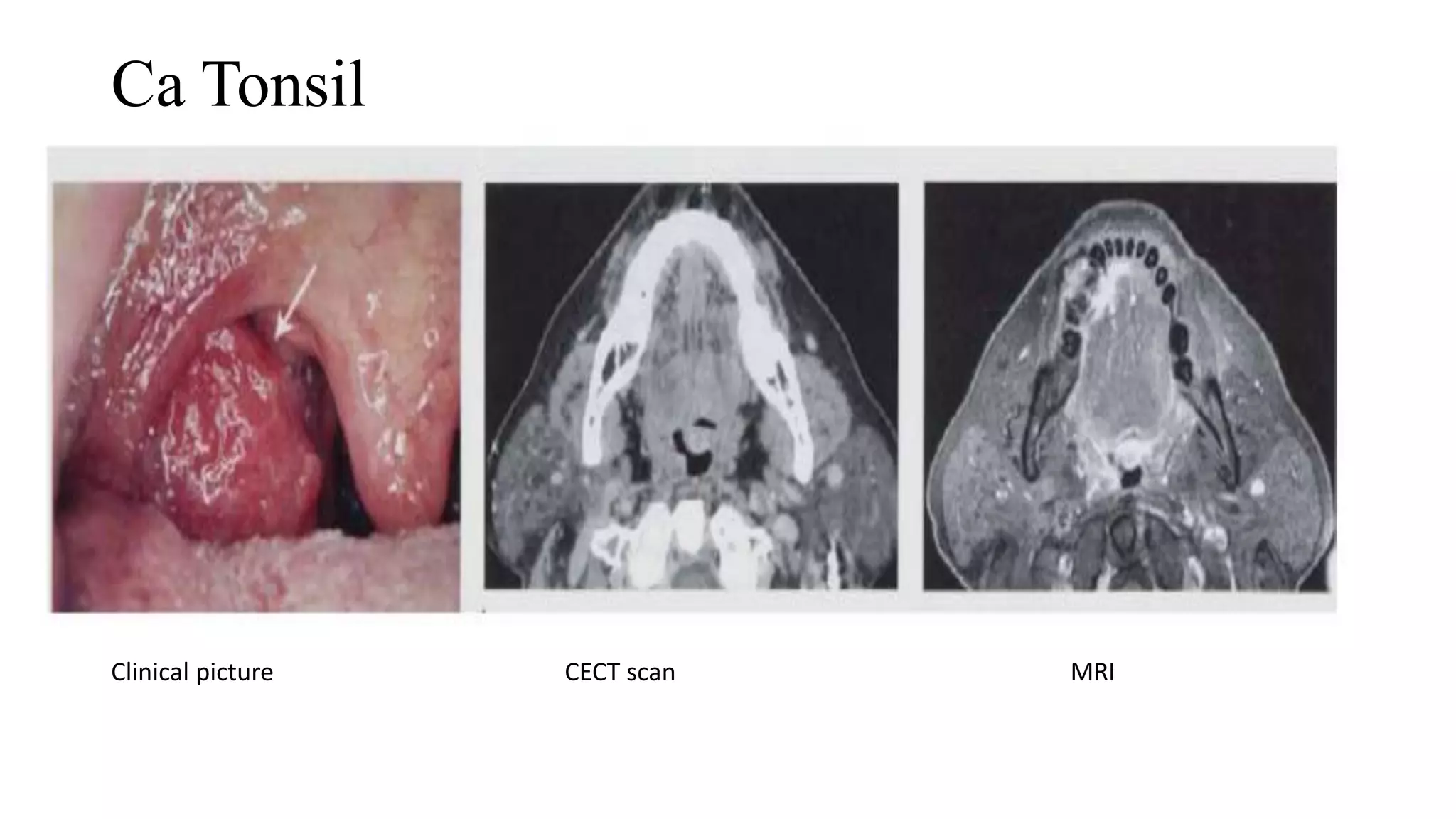
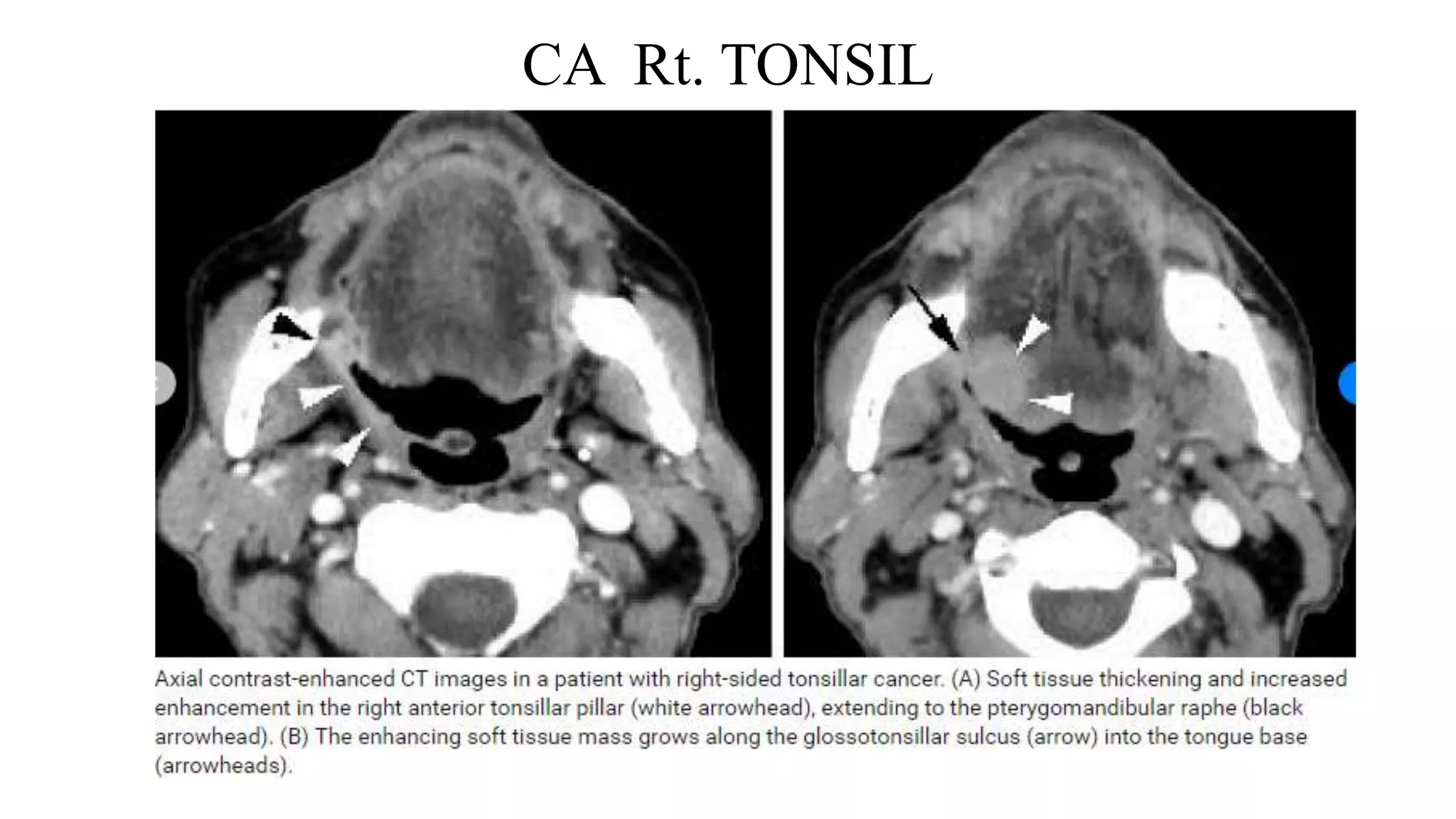
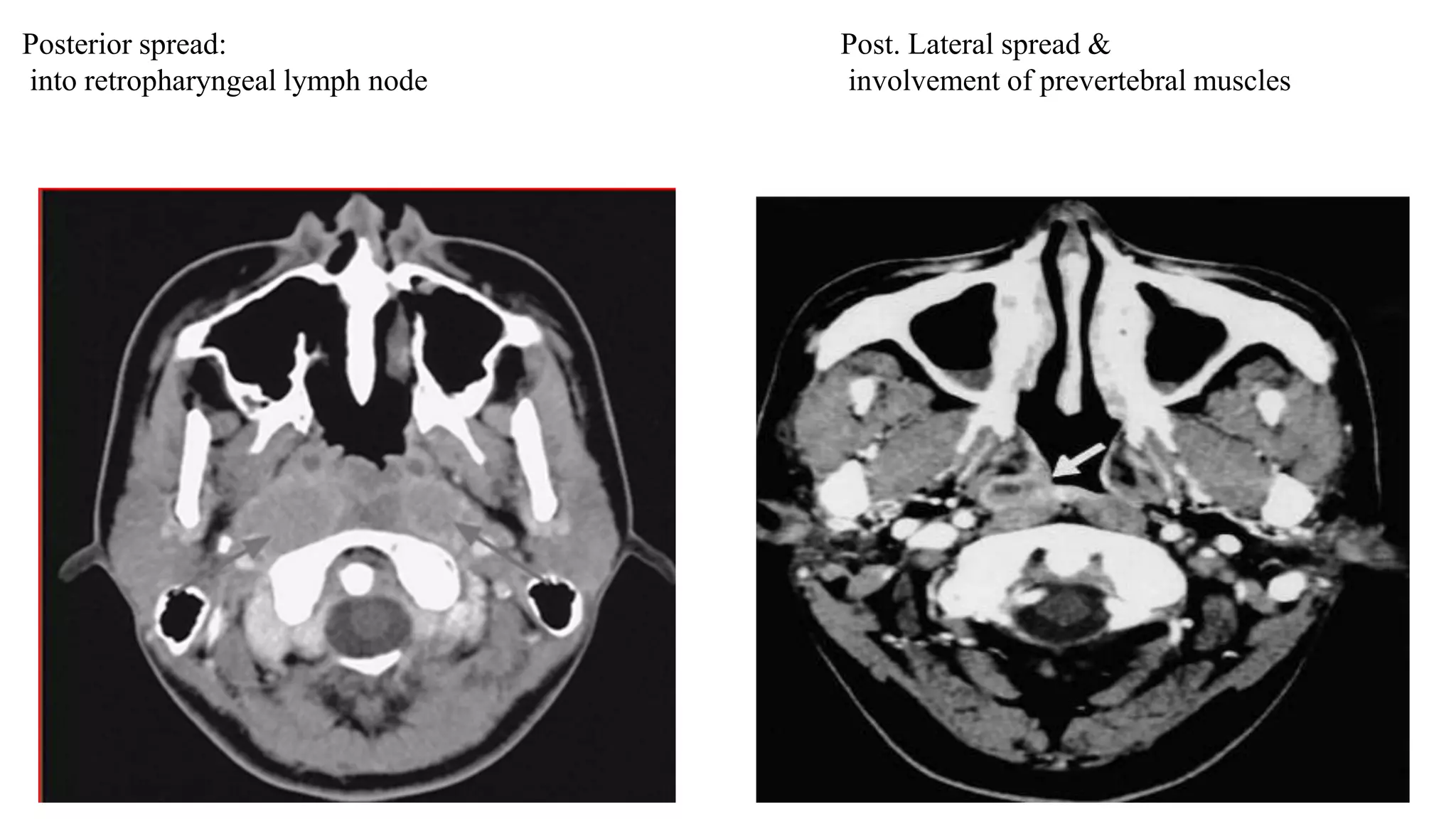
Radiological findings for oropharyngeal cancers, detailing anatomical structures and imaging results.Anatomy of the nasopharynx and typical cancer presentations including patterns of spread.
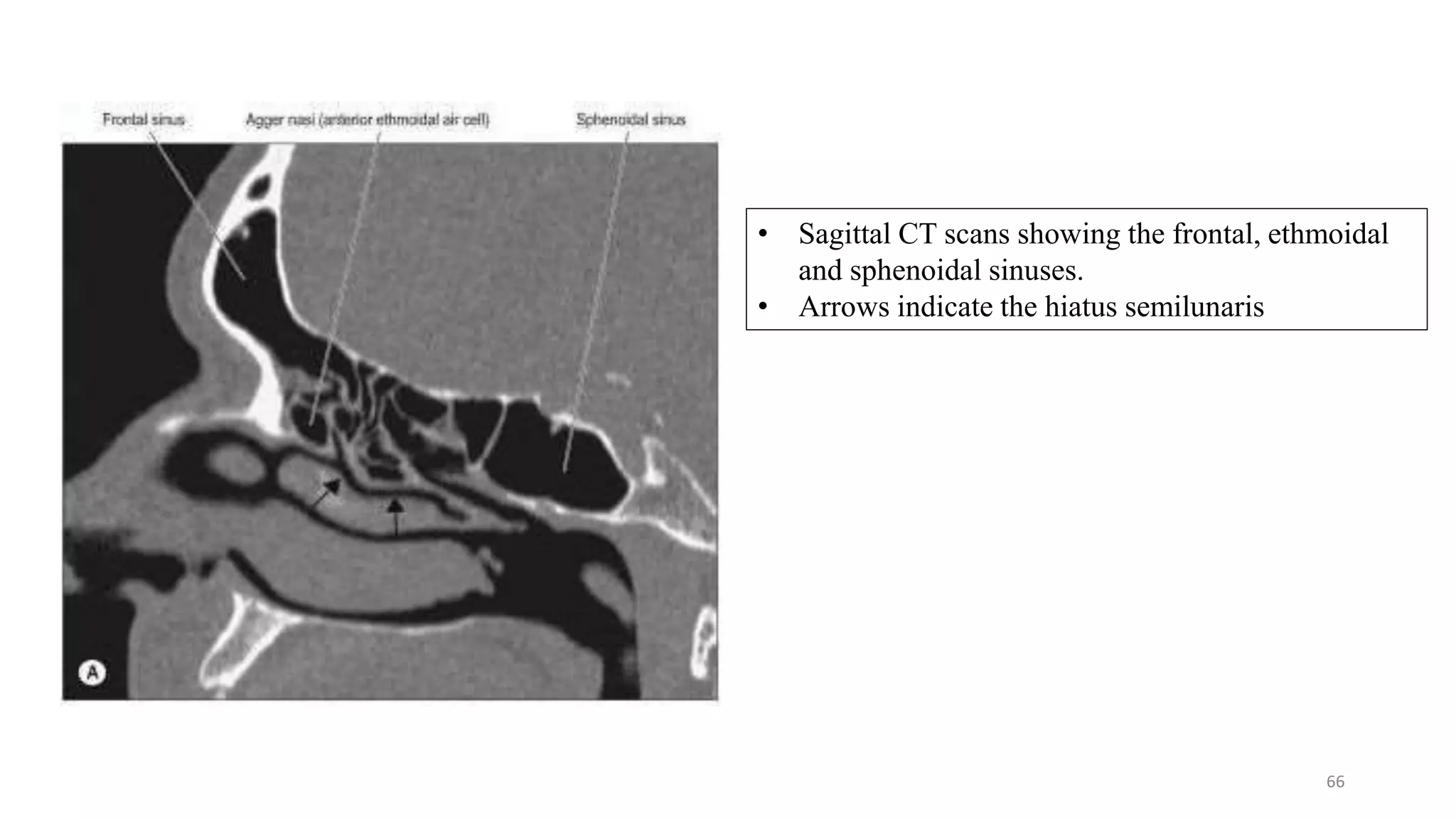
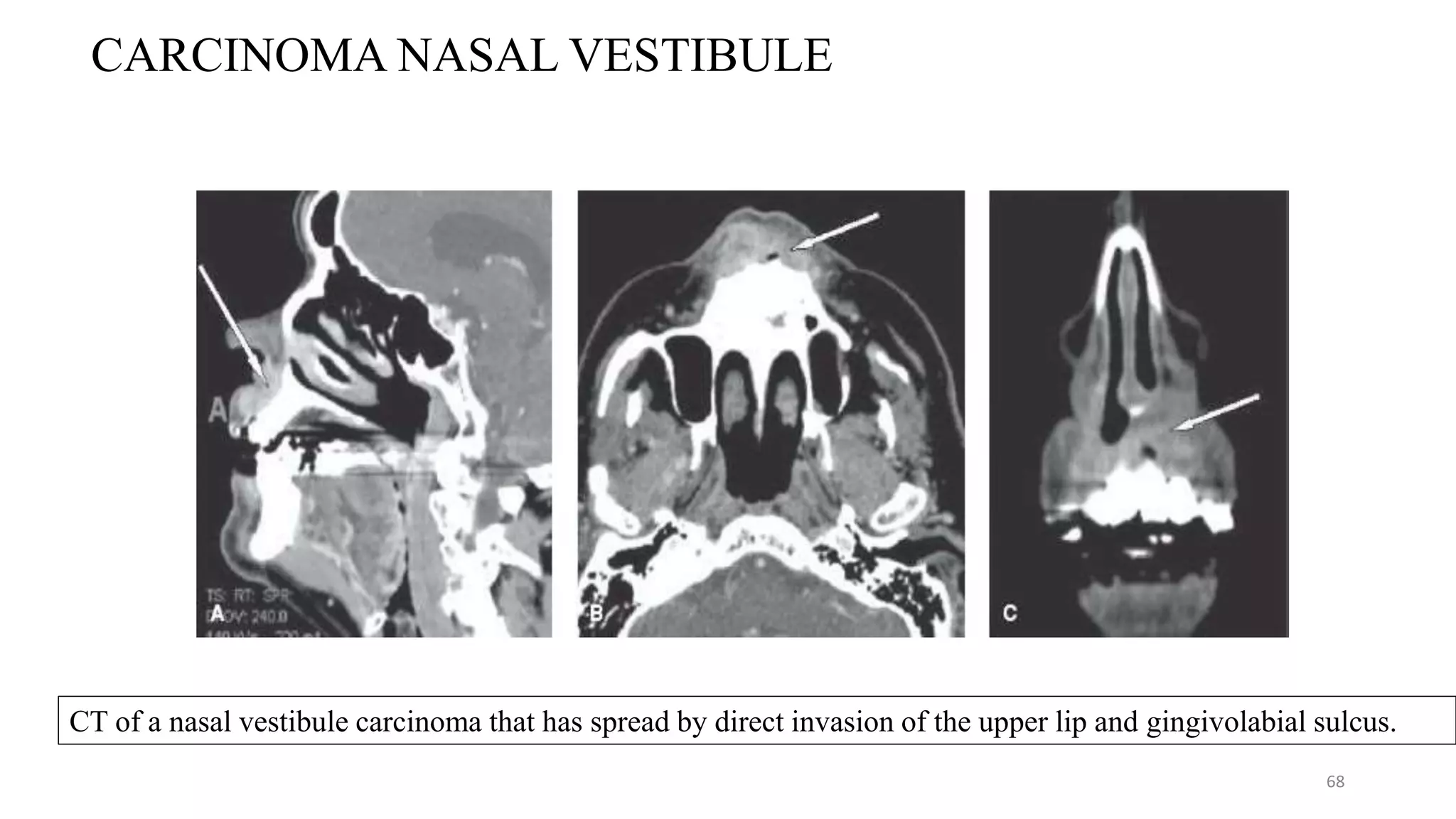
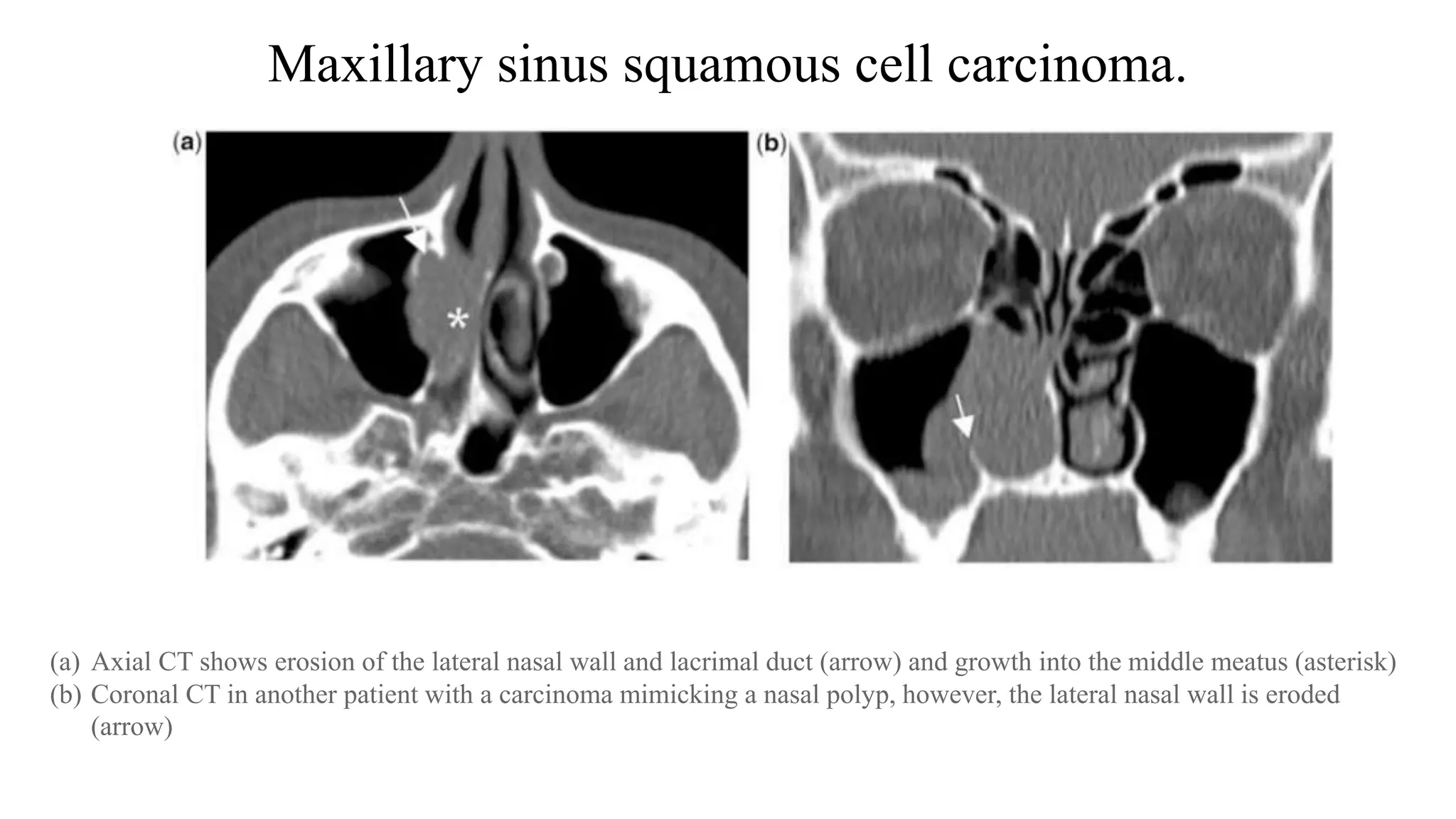
Radiological anatomy of the nasal cavity and sinuses along with cancer manifestations and assessment.
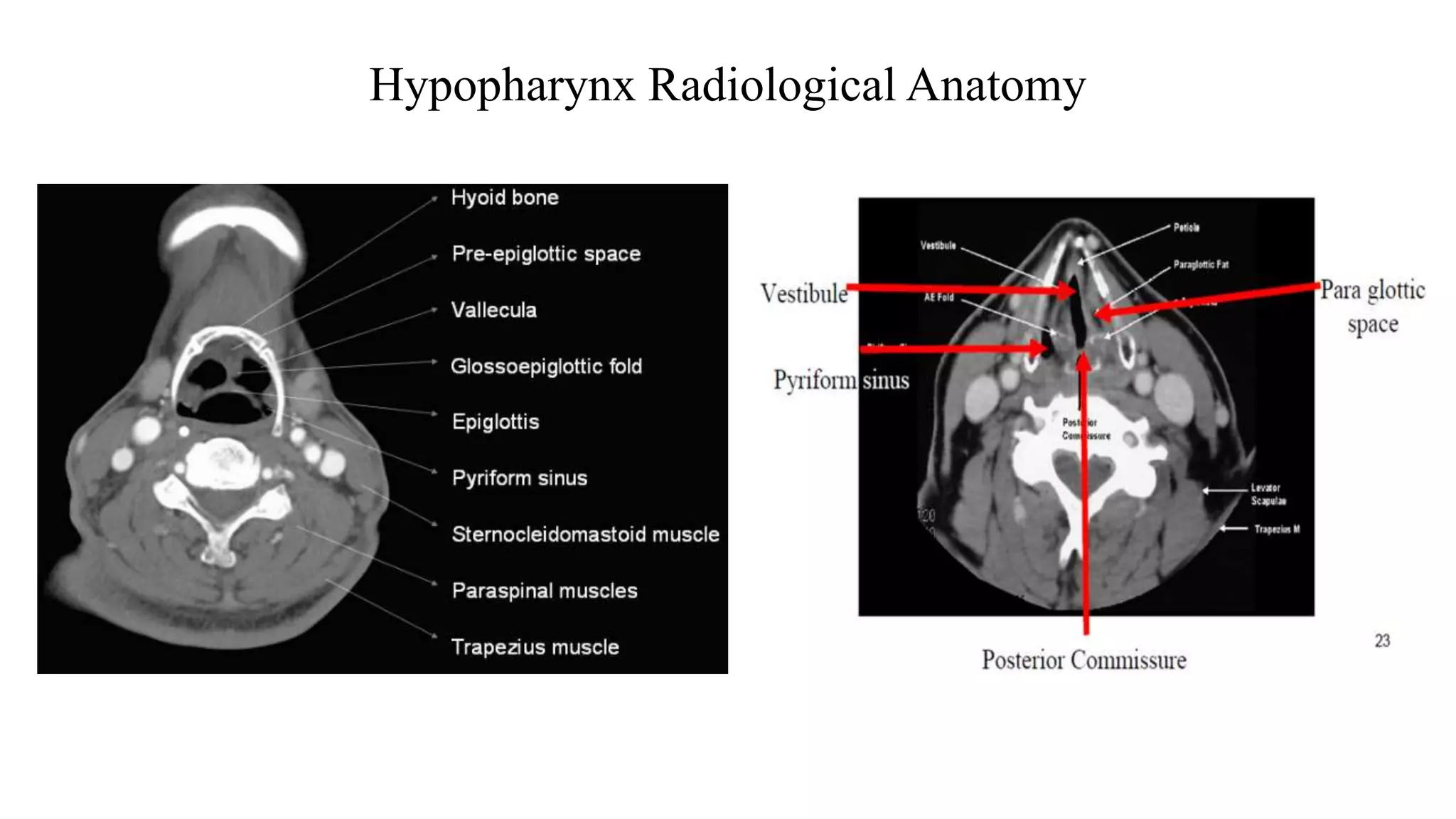
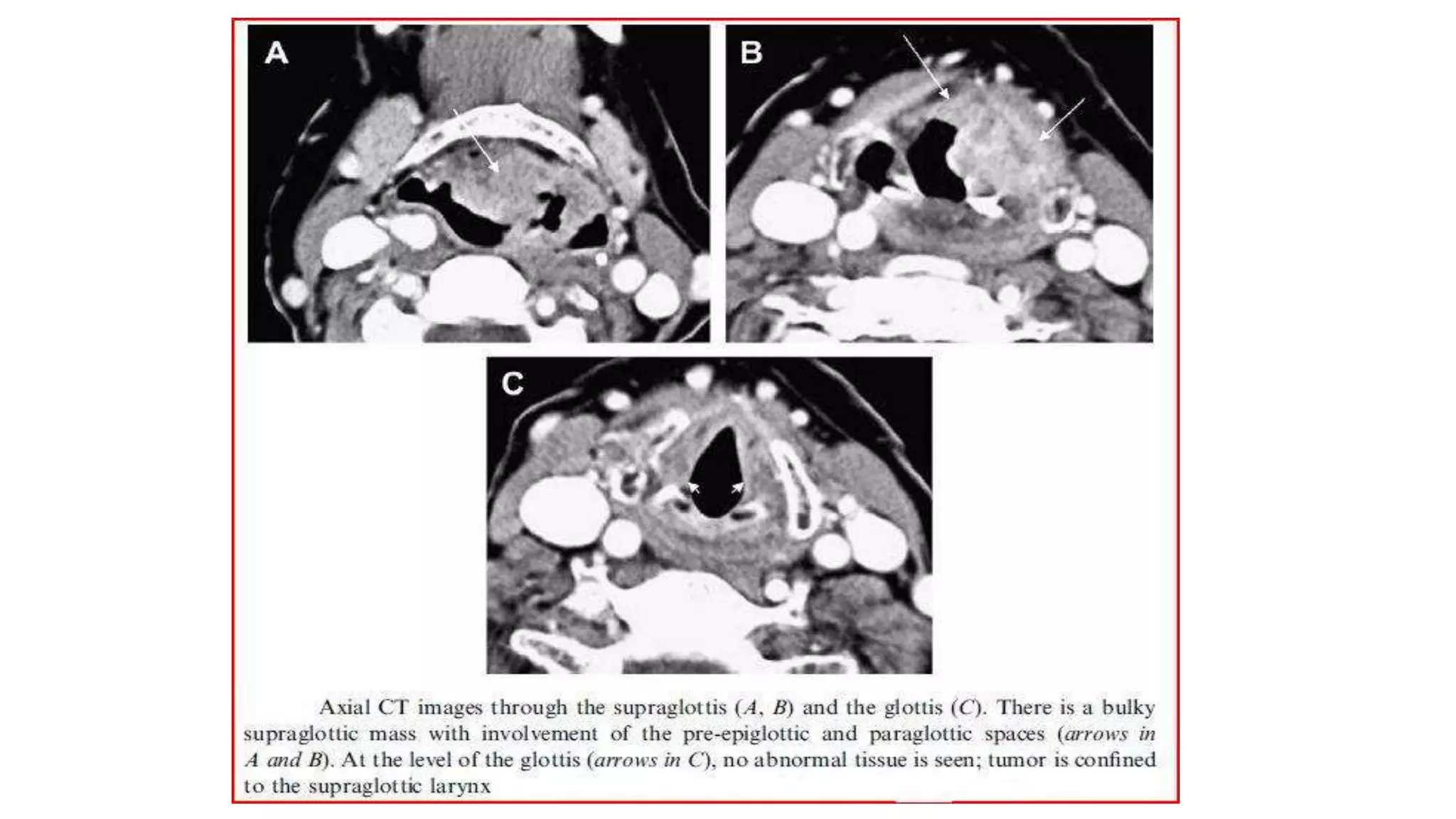
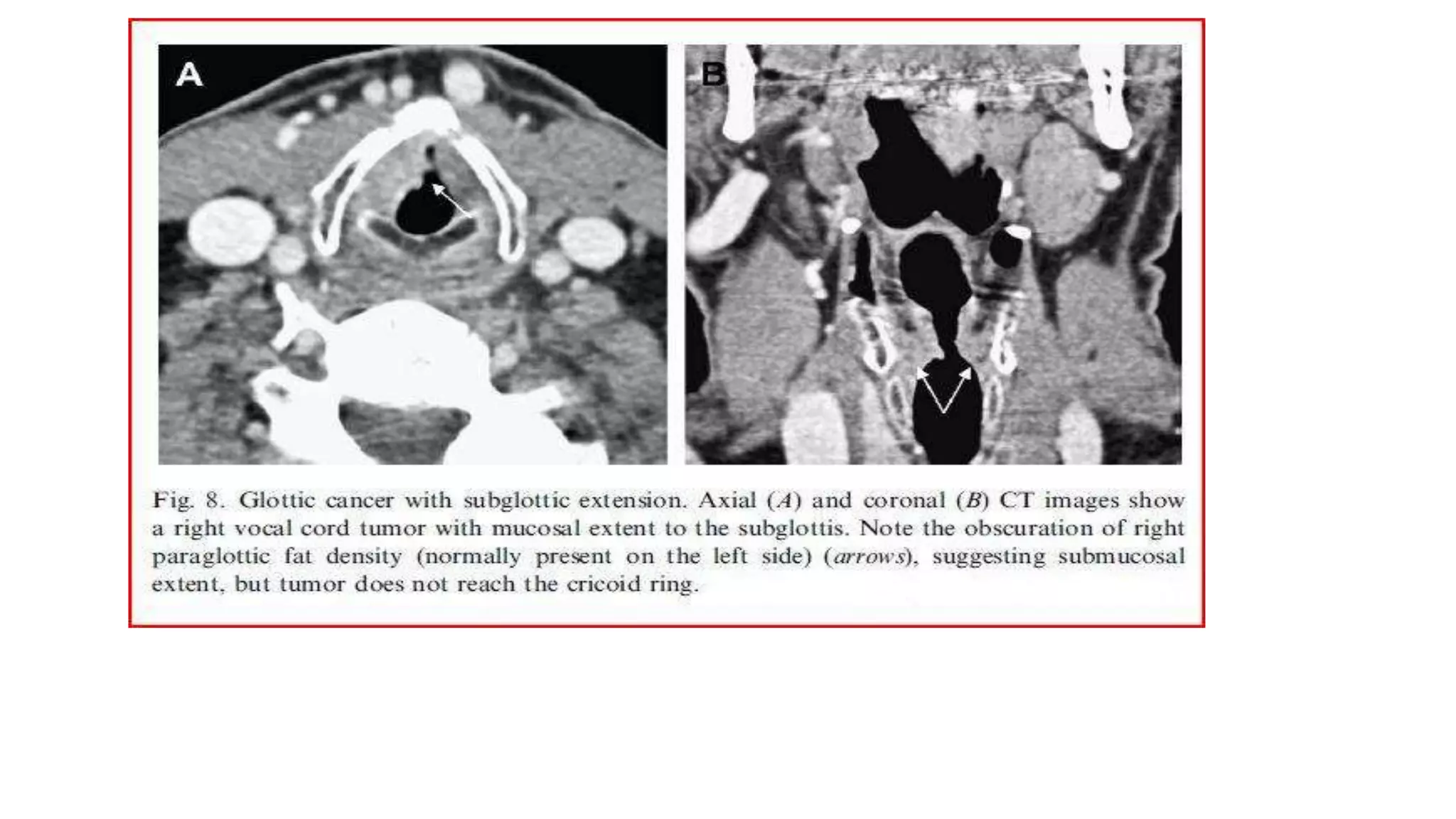
Radiological characteristics and assessment of hypopharyngeal cancers.
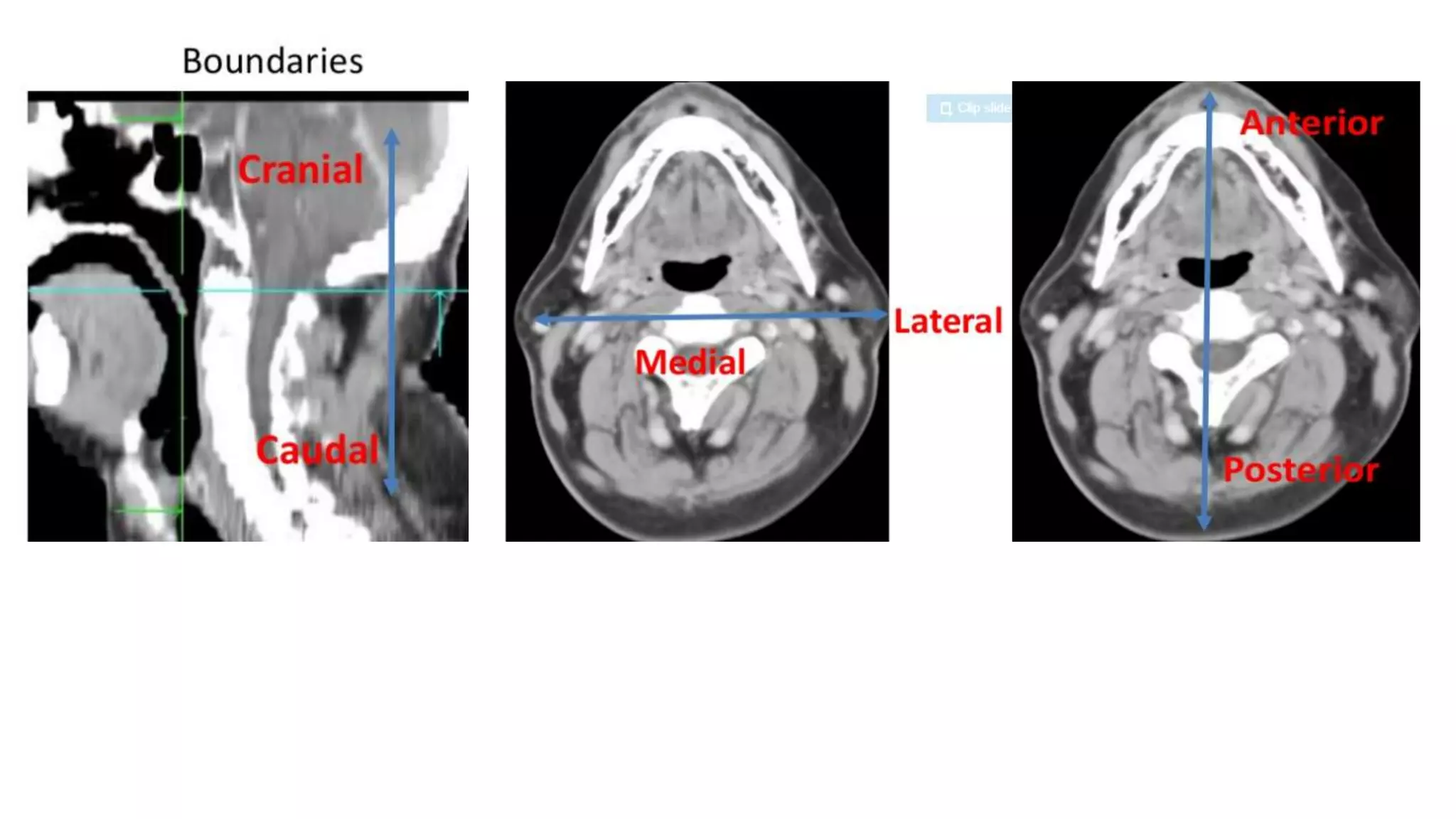
Anatomy, boundaries, and implications of enlarged lymph nodes in head and neck cancers.














![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)








































































