



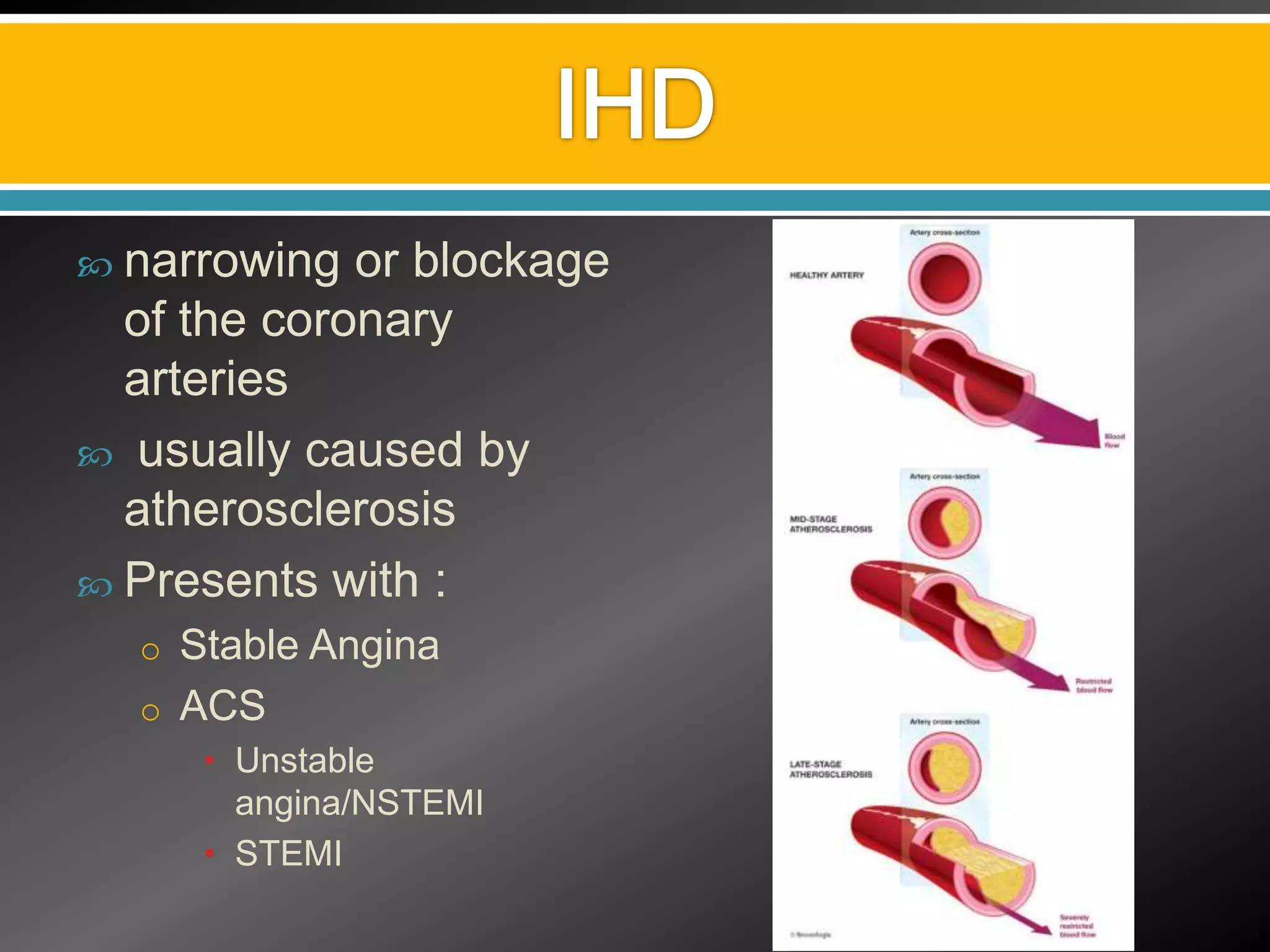






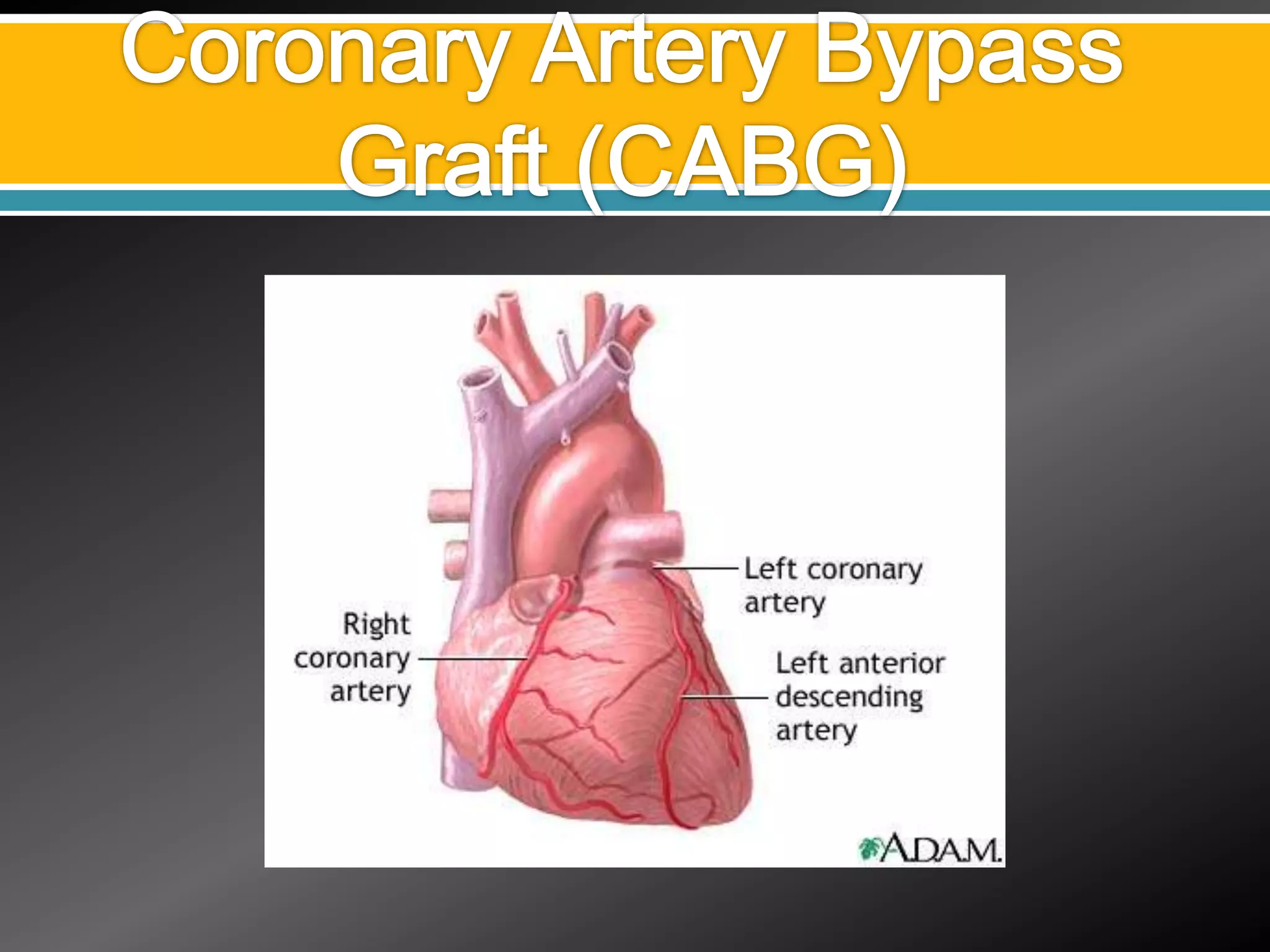












This document discusses various aspects of ischemic heart disease (IHD) including: 1) Causes, symptoms, and diagnostic tests for IHD including angiography, echocardiography, and exercise ECG. 2) Treatment options for IHD including medical management, percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), and off-pump CABG. 3) Surgical complications of IHD and their management through procedures like mitral valve repair, ventricular septal defect repair, and left ventricular aneurysm repair.



















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













