Downloaded 340 times
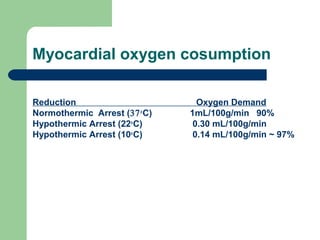
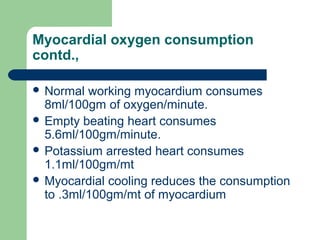
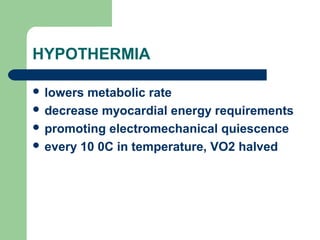
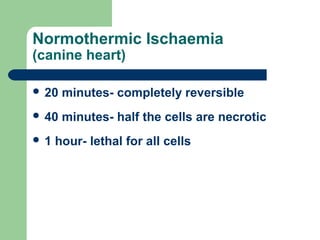


This document discusses various strategies for myocardial protection during cardiac surgery. It describes how ischemia and reperfusion injury can damage the myocardium. The goals of myocardial protection are to reduce oxygen demand, maintain adequate perfusion, and minimize injury during reperfusion. Techniques discussed include cardioplegic arrest, hypothermia, venting, intermittent clamping, and pharmacological additives to cardioplegia solutions. The optimal method balances protection against procedural complexity and aims to prevent intraoperative damage and ensure postoperative cardiac function.






































![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![heart surgery [Autosaved].pptx ppppppptt](https://cdn.slidesharecdn.com/ss_thumbnails/autosaved-241123170357-8bf931d7-thumbnail.jpg?width=640&height=640&fit=bounds)















































