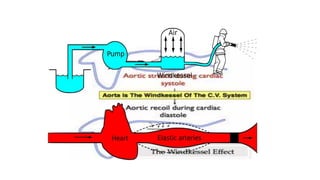
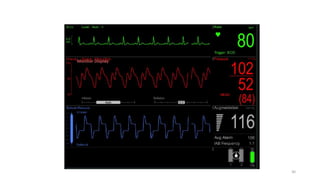
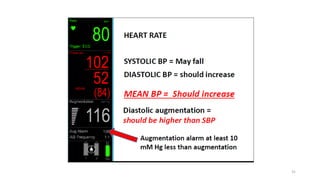
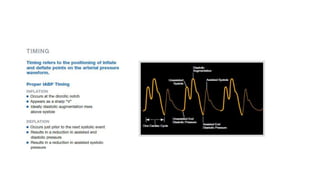
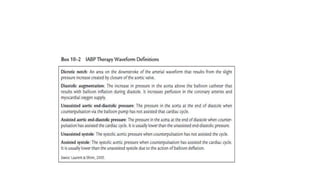
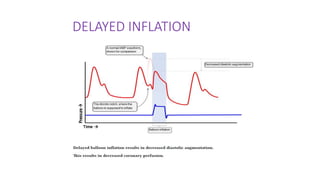
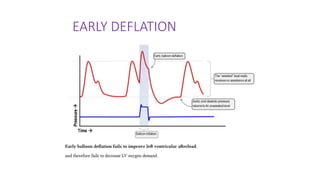
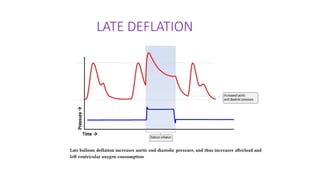
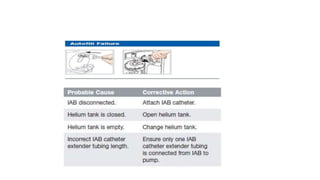
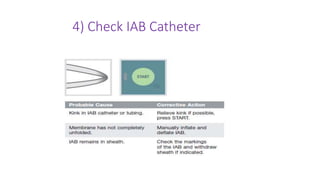
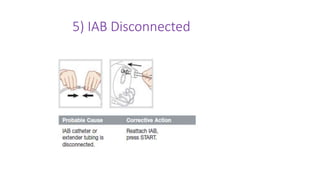
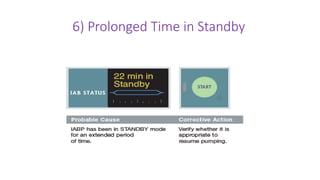
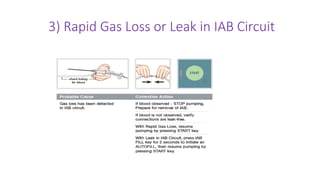
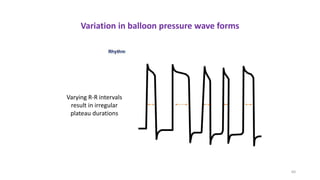
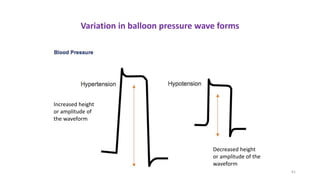
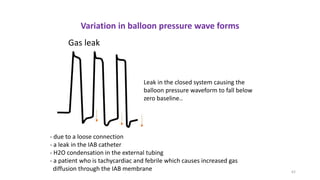
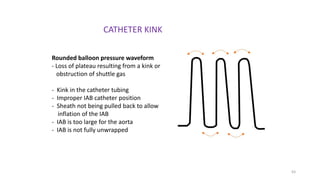
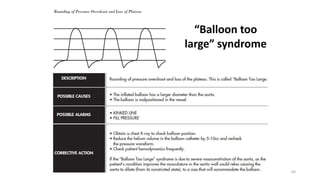
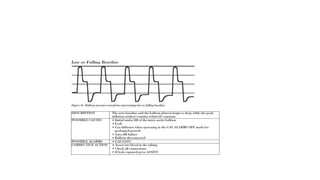
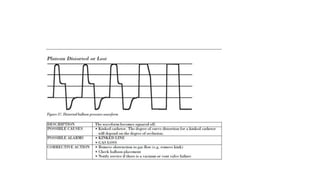
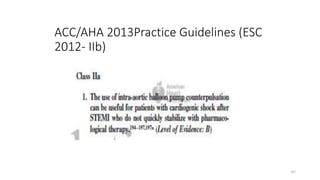
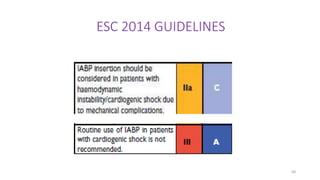
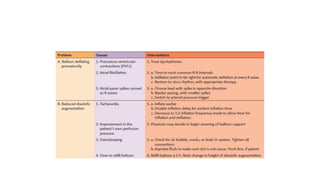
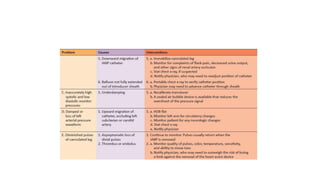
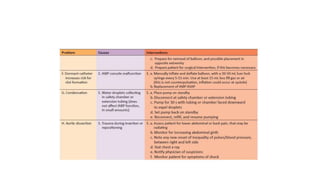
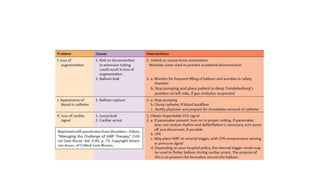
The document discusses intra-aortic balloon pump (IABP) troubleshooting. IABPs are used to improve cardiac function in patients awaiting procedures like bypass surgery. They work by inflating in diastole to increase blood flow and deflating in systole to reduce workload on the heart. Common issues include low augmentation due to timing errors, leaks, or poor function. Other problems involve lack of ECG trigger, autofill failure, catheter kinks, or disconnects. Understanding potential issues helps optimize IABP therapy for cardiogenic shock patients.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

