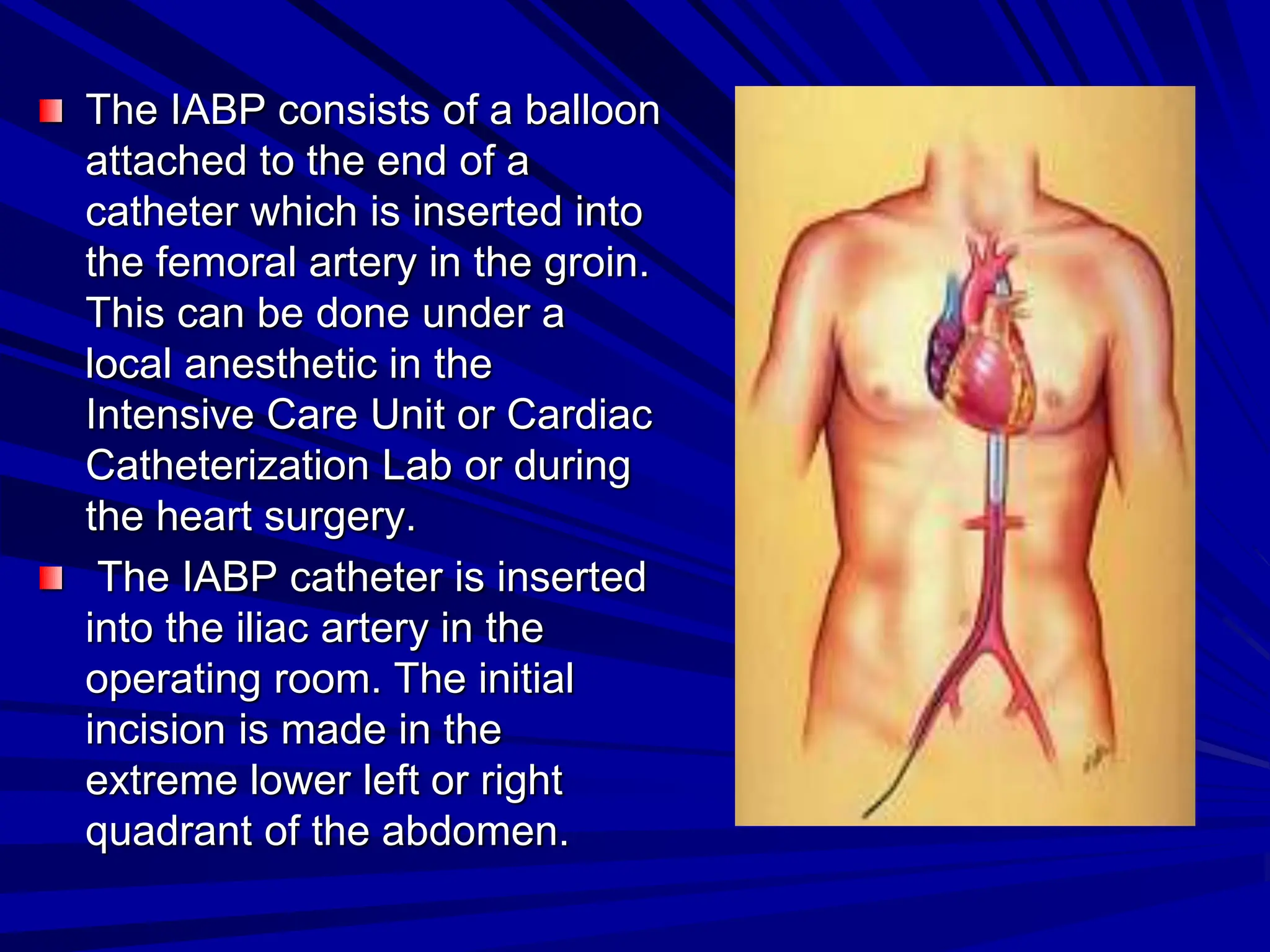
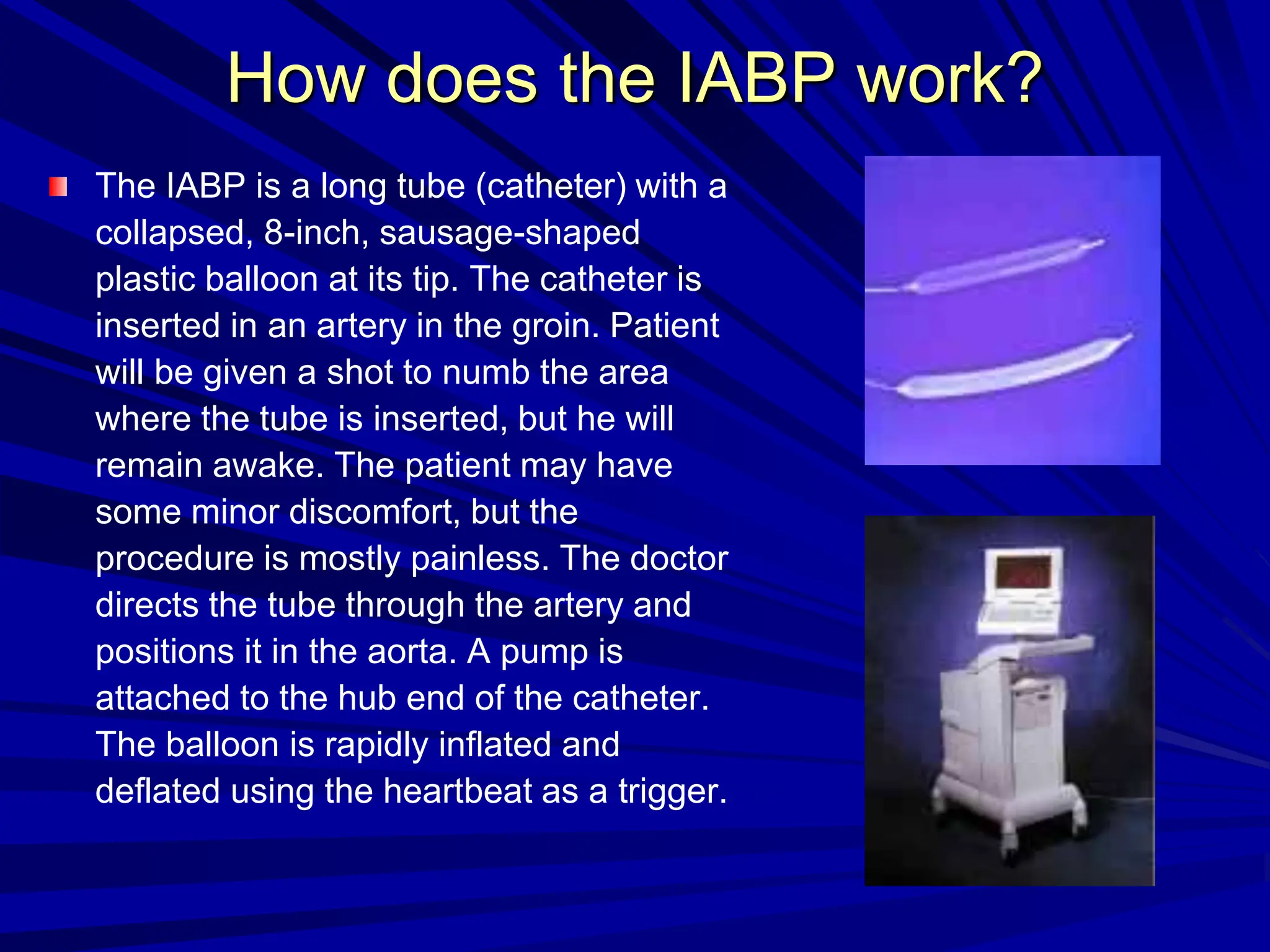
The intra-aortic balloon pump (IABP) is a device placed in the aorta to help the heart pump more effectively by increasing blood flow and decreasing workload. It consists of a balloon on a catheter inserted into the femoral artery. The balloon inflates during heart relaxation and deflates before contraction to alter pressure and blood flow. IABP can help in heart failure, heart attack, or for patients awaiting transplantation. Potential complications include infection, bleeding, or limb ischemia requiring removal. Nurses monitor patients closely for complications and make frequent assessments of pulses, dressings, and output.