Downloaded 504 times
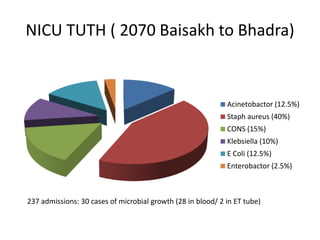
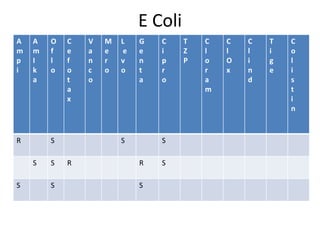
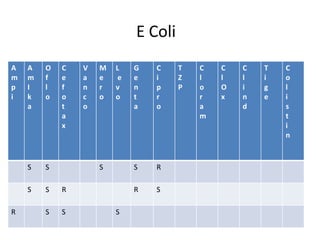
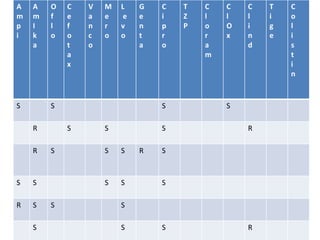
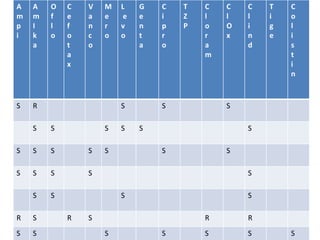
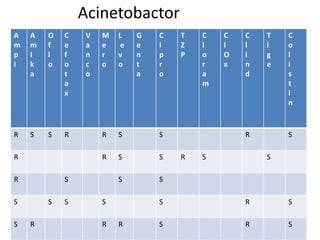
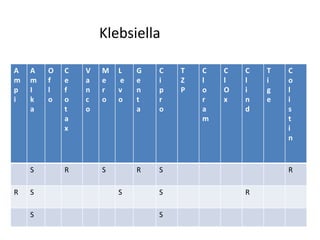
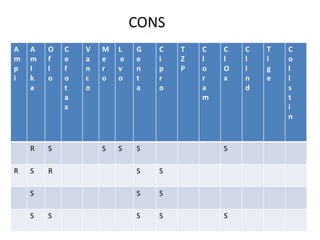
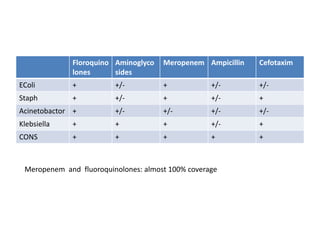
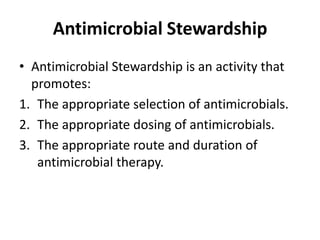
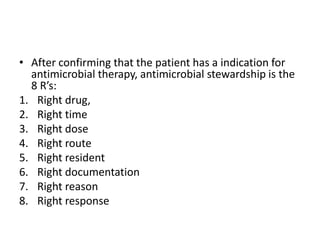
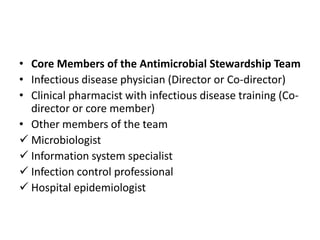
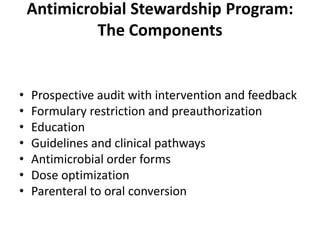
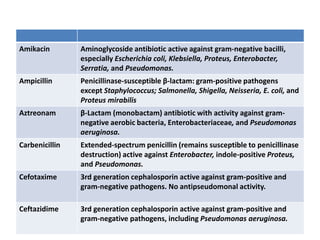
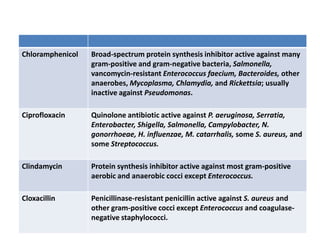
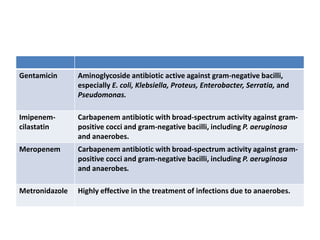
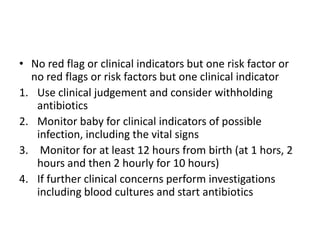
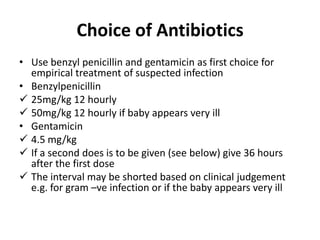
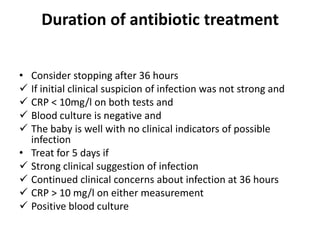
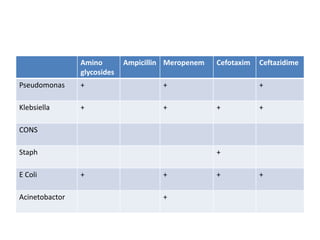
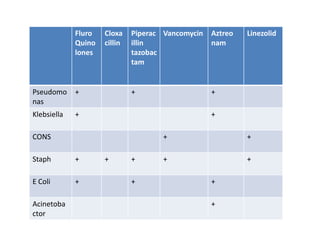

The document discusses the importance of rational antibiotic use in newborns, highlighting the consequences of incorrect use, including antimicrobial resistance and adverse drug reactions. It emphasizes that appropriate medicine use requires correct dosage and duration while addressing factors that contribute to misuse, such as lack of knowledge and unethical pharmaceutical promotion. The text also outlines strategies to improve antibiotic stewardship and summarizes data on bacterial resistance patterns and antibiotic susceptibility in neonatal care settings.
































































































