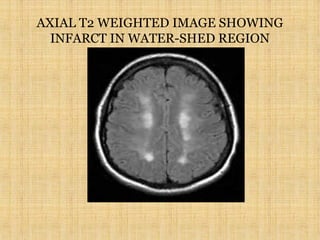
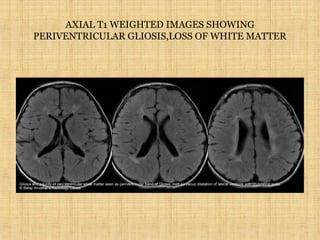
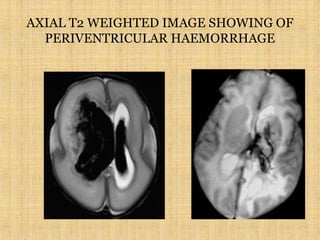
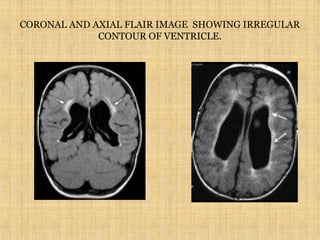
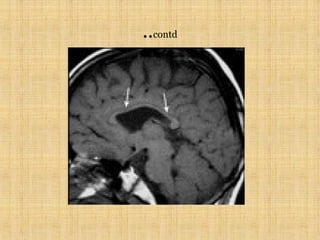
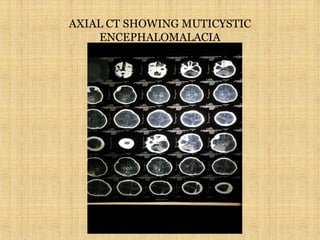
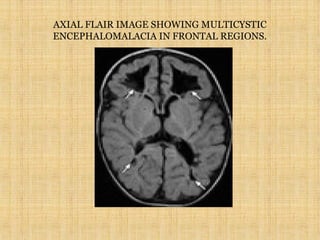
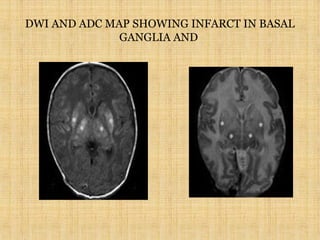
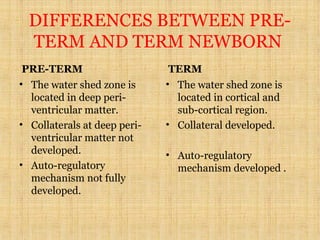
Hypoxic ischemic encephalopathy (HIE) results from global reduction in blood flow, oxygen, or glucose to the brain. It depends on gestational age, duration of insult, and collateral circulation. In term infants, injury occurs in cortical and subcortical watershed zones, while preterm infants experience injury in deep periventricular white matter. Imaging findings include infarction, hemorrhage, edema, and in severe cases, multicystic encephalomalacia. Outcomes range from full recovery to death, with preterm infants having a worse prognosis. Treatment focuses on supportive care, seizure control, and managing brain edema. HIE remains an important cause of neonatal mortality and long-term neurological impairments