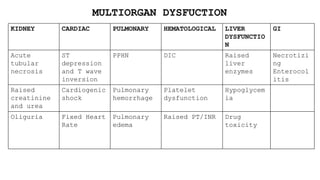
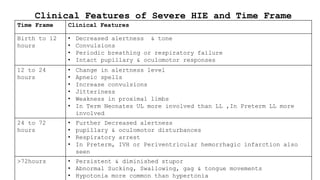
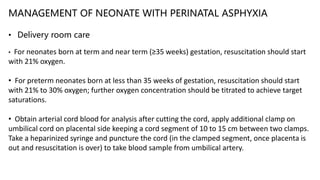
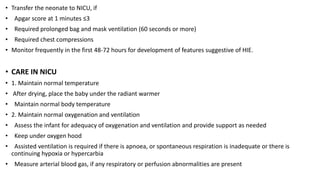
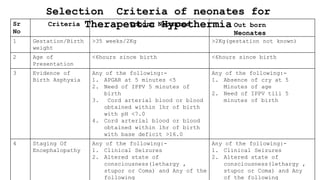
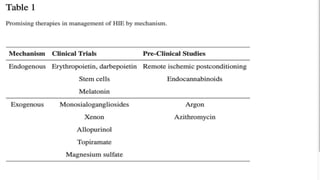
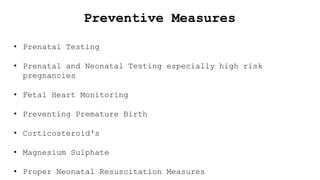
Hypoxic ischemic encephalopathy (HIE) is a serious brain injury caused by oxygen deprivation and is majorly due to birth asphyxia, resulting in significant neonatal mortality. Diagnosis relies on clinical signs, laboratory tests, and imaging techniques, while management includes supportive care and therapeutic hypothermia for eligible neonates within the first hours of life. Preventive measures focus on prenatal care and timely intervention to avoid complications and improve outcomes for affected infants.


















![Community acquired pneumonia [cap] in children](https://cdn.slidesharecdn.com/ss_thumbnails/communityacquiredpneumoniacap-130907093236--thumbnail.jpg?width=640&height=640&fit=bounds)














































