
Downloaded 22 times
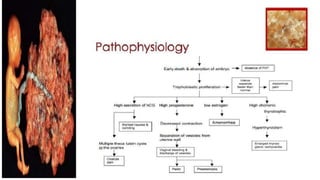
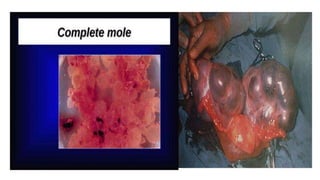
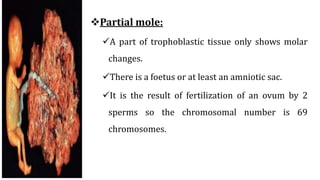


This document defines and describes hydatidiform mole, a benign tumor of the chorionic villi that can develop during early pregnancy. It discusses the two types of molar pregnancies - complete and partial mole - and their causes. Common symptoms include amenorrhea, vomiting, and vaginal bleeding. Diagnosis is typically made through an elevated hCG level in urine and ultrasound showing a snowstorm appearance. Surgical evacuation is the main treatment, with follow up to monitor hCG levels for potential choriocarcinoma development. Nursing care focuses on pain management, hygiene, emotional support, and monitoring for complications like hemorrhage and infection.














































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)








