This document discusses hydratidiform mole, also known as vesicular mole, which is an abnormal condition of the placenta characterized by degenerative and proliferative changes in the chorionic villi resulting in clusters of cysts. It has the highest incidence in Asia and occurs more commonly in teenagers and women over 35. Complete moles show only paternal chromosomes while partial moles contain some fetal tissue. Management involves supportive care, surgical evacuation of the uterus, and long-term monitoring of hCG levels to detect persistent trophoblastic disease.
Pathology of Ectopic pregnancy, spontaneous abortion and gestational trophobl...Sufia Husain
DISORDERS OF PREGNANCY AND PLACENTA.
Pathology of ECTOPIC PREGNANCY, SPONTANEOUS ABORTION AND GESTATIONAL TROPHOBLASTIC DISEASE for medical and health care students
Pathology of Ectopic pregnancy, spontaneous abortion and gestational trophobl...Sufia Husain
DISORDERS OF PREGNANCY AND PLACENTA.
Pathology of ECTOPIC PREGNANCY, SPONTANEOUS ABORTION AND GESTATIONAL TROPHOBLASTIC DISEASE for medical and health care students
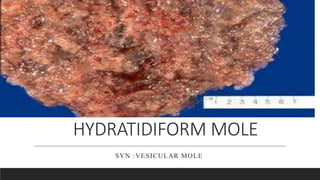
It is an abnormal condition of the placenta where there are partly degenerative and partly proliferative changes in the young chorionic villi. These result in the formation of clusters of small cysts of varying sizes. Because of its superficial resemblance to hydatid cyst, it is named as hydatidiform mole.
Ectopic Pregnancy - Obstetrical & Gynaecological NursingJaice Mary Joy
In ectopic pregnancy, implantation occupies at a site other than the endometrium. Ectopic pregnancies are responsible for approximately 10 percent of all maternal mortality. The prognosis for future reproduction is poor. Only one half of women having an ectopic pregnancy are eventually delivered of a liveborn infant. Various factors contribute to ectopic pregnancies, the most common being infection. Unlike intrauterine spontaneous abortions, genetic factors are not paramount in the etiology of ectopic pregnancy.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
2. Introduction
It is an abnormal condition of the placenta where they are
partly degenerative and partly proliferative changes in the
young chorionic villi.
These result in the formation of the clusters of the small
cysts of varying size.
3. Introduction contd……
Because of its superficial resemblance to hydratid cyst, it is
named as hydratidiform mole.
It is best regardes as a benign neoplasia of the chorion with
malignant potential.
4. Incidence
There is a wide range of geographical and ethnic variation
of the prevalence of the condition . It is more common in
China, Indonesia ,Japan.
Highest in philippines-1 in 100 pregnancy
Lowest in European countries(USA)-1in 2000
Incidence in India –1 in 400
6. Classification
Partial mole
• Some fetal tissue ,blood vessels and villi present
Complete mole
• No fetal tissue , blood vessels and villi formation
7. Etiology
The cause is not definitely known ,but it appears to be
related to the ovular defect as it sometimes affects one ovum
of a twin pregnancy .however, the following faactors and
hypothesis have been forwarded:
8. Etiology contd..
Its prevalence is higher in teenagers and in women aged
beyond 35 years.
The prevalence appears to vary with race and ethnic group
Inadequate intake of protein , carotene and high intake of
animal fat specially in oriental countries.
Imbalance immune mechanism eg in hepatic disease rise in
gamaglobuline ,AB blood group.
9. Etiology contd.....
Cytogenetic abnormalities
The higher the ratio of paternal :maternal chromosomes,
the greater is the molar change . Complete mole show 2:1
ratio
History of prior hydratidiform mole increases the chance of
recurrence(1 to 4%).
11. Pathophysiology contd…..
Death of the ovum or failure of the embryo to grow is
essential to develop complete hydratidiform mole
The secretion from hyperplastic cells and transferred
substances from the maternal blood accumulate in the
stroma of the villi
Results in the distension of the villi to form vessicles
14. b. vomitting become excessive
c.breathlessness due to pulmonary embolism of trophoblastic
cell
Expulsion of grapes like vesicles per vagina is diagnose of
vesicle mole
History of quickening is absent
15. Sign
Feature suggestive of early months of pregnancy are
evident
The patient look more ill than can be accounted for.
Pallor is usually prominent ,out of the proportion of the
visible blood loss
16. Feature of preeclampsia due to the hyperactivity of the
trophoblastic cells
Per abdomen :
The size of the uterus : larger
The feel of the uterus : firm elastic
Fetal parts: not palpable
Absence of fetal heart sound
17. Vaginal examination
Internal ballottement can not be elicited
Finding of the vesicles in the vaginal discharge
If cervical os is open, instead of membranes,blood clot or
the vesicles may be felt.
18. Investigations
Full blood count ,ABO and Rh typing
Hepatic ,renal and thyroid function are carried out
Sonography:
Qualitative estimation of chorionic gonadotrophin
Straight X- ray abdomen
CT and MRI
Beta –hCG estimation
20. Complication
Haemorrhage and shock due to vaginal bleeding over a
time
Sepsis – inccrease the chances of ascending infection due
to blood clot ,vaginal bleeding and absence of fetal
membrane
Uterine perforation – due to invasive mole or surgical
procedure
21. Complication contd…..
Gestational trophoblastic disease – it may develop
persistently elevated beta –hCG and may lead to
choriiocarcinoma
Recurrence – there are chances of recurrence of the mole in
subsequent pregnancies.
22. Management
The principle of management are :
Supportive therapy to restore the blood pressure and
infection
Evacuation of the uterus as soon as diagnosis is made
Counselling for regular follow up to detect the persistent
trophoblastic disease
23. Management Contd…
1.supportive management
Group A – the patient usually presents with various amount
of bleeding :
to starts a ringers solution I.V. infusion
Arrangement is made for blood transfusion
25. Management contd…...
2. Definitive management :
Suction evacuation (it is the treatment of choice
irrespective of the uterine size)
suctioning with manual vacuum aspiration is safe, which
should be done rapidly. The risk of perforation is high in
using metal curettage.
26. Management contd…
digital exploration and removal of the mole by ovum
forceps may helpful to evacuate the content of the uterus.
Infuse oxytocin 20 unit in 1 liter IV fluids (NS or RL) at 60
drops per minute to prevent hemorrhage once evacuation is
under way.
Administration of Rh ( D) immunoglobulin to women who
are Rh negative to prevent isoimmunization
27. Management contd……
Hysterotomy : the procedure are rarely done. The
indications are;
Profuse vaginal bleeding
Cervix unfavourable for immediate vaginal evacuation
28. Management contd…
Hysterectomy :this is indicated in;
Patient with age over 35
High risk patient with development of future malignancy
Female has completed her family irrespective of age
Perforating mole
Placental site trophoblastic tumor
29. Management contd….
2. Follow up management:
Routine follow up is mandatory for all cases for at least 6
months following molar pregnancy.
first B- hCG level is obtained 48 hours after evacuation
Then monitor serum hCG levels every weekly till they
become normal for three consecutive weeks.
30. Management contd….
Once the hCG levels falls to a normal level for 3 weeks,
test the patient monthly for 6 months; then follow- up is
discontinued and pregnancy allowed.
During the 6 month surveillance period, patient is advised
not to become pregnant.
31. Contraceptive advice
Contractive of choice being combined oral pills
IUD is contraindicated, because of its frequence
association of the irregular bleeding
Inj. DMPA can be used safely
surgical sterilization is another alternative when family
size is complete