
Download to read offline

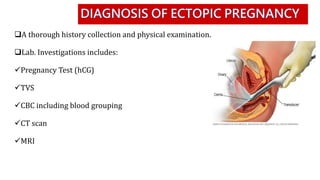
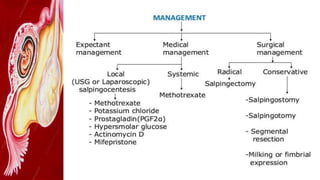

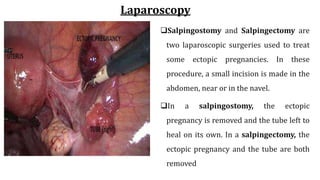

Ectopic pregnancy, occurring in 1-2% of pregnancies, happens when a fertilized egg implants outside the uterus, commonly in a fallopian tube. Diagnosis involves history, blood tests, and imaging, with management options including expectant management, medical treatment with methotrexate, or laparoscopic surgery depending on the condition's specifics. Risk factors include previous ectopic pregnancies, infections, and certain reproductive health conditions.























































































