Downloaded 42 times

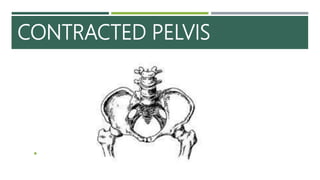
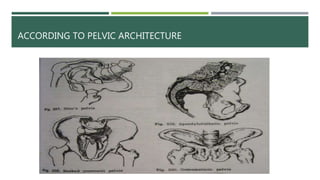
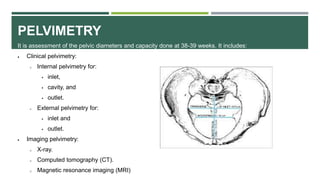
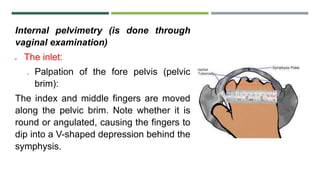
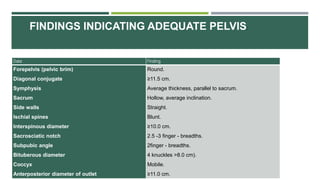
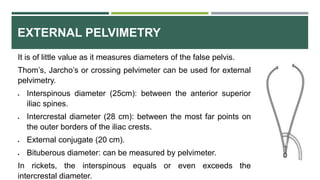
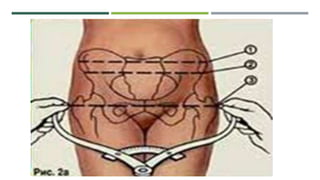


Contracted pelvis, also known as pelvic disproportion, occurs when the essential diameters of the pelvis are shortened, altering the normal mechanism of labor. It can be caused by developmental, metabolic, traumatic or other factors. Pelvises are classified based on degree of contraction and pelvic architecture. Diagnosis involves history, physical exam including internal and external pelvimetry, and sometimes radiological imaging. An internal pelvimetry exam evaluates the inlet, cavity, and outlet to determine pelvic adequacy for vaginal delivery.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




