Download to read offline

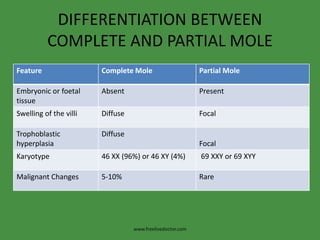



Hydatidiform mole is a benign tumor of the chorionic villi that can develop during early pregnancy. It occurs more frequently in Asia and in women over age 45. A complete mole contains no embryo and develops from fertilization of an empty ovum by one sperm, while a partial mole contains some fetal tissue and develops from double fertilization of one egg. Diagnosis is based on vaginal bleeding, elevated hCG levels, and ultrasound findings, while treatment involves surgical evacuation of the uterus. Patients require long-term follow-up to monitor for choriocarcinoma, a rare type of cancer that can develop after a molar pregnancy.















































