
Downloaded 26 times
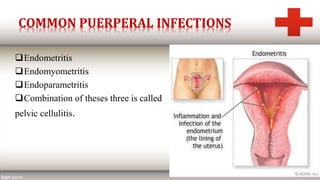
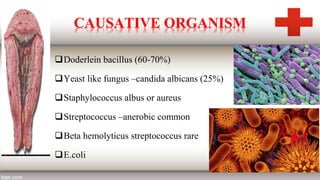
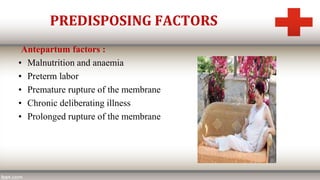
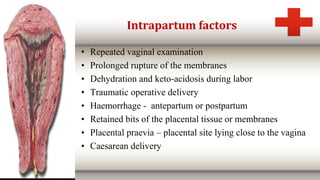

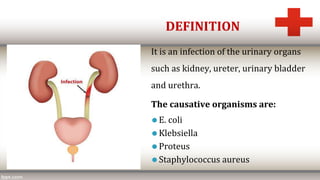


The document discusses puerperal sepsis and urinary tract infections. Puerperal sepsis is defined as an infection of the genital tract occurring after childbirth. Common causes include bacteria like Doderlein bacillus. Risk factors include prolonged rupture of membranes, operative deliveries, and retained placental tissues. Signs include fever, foul-smelling discharge, and pelvic pain. Treatment involves isolation, intravenous antibiotics like cefotaxime and metronidazole, and possible drainage of abscesses. Urinary tract infections in the postpartum period are also discussed, with E. coli being a common cause. Symptoms include fever and painful urination. Diagnosis is by urine culture and























































































