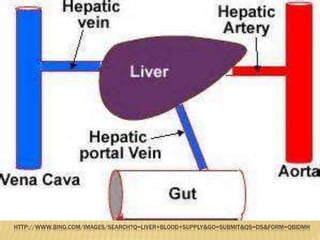
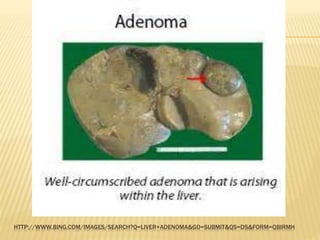
This document provides an overview of hepatic and pancreatic tumors. It discusses the clinical anatomy and physiology of the liver and pancreas. It describes different types of benign hepatic tumors like hemangiomas, adenomas, and focal nodular hyperplasia. For malignant hepatic tumors, it discusses hepatocellular carcinoma and cholangiocarcinoma. It covers the epidemiology, investigations, and management options for these tumors. For the pancreas, it discusses anatomy, physiology, tumor types including neuroendocrine tumors, and the management of pancreatic tumors through surgery or palliation.

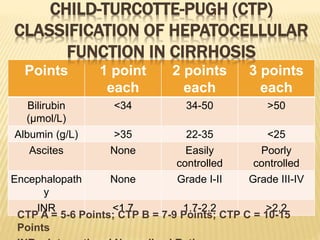
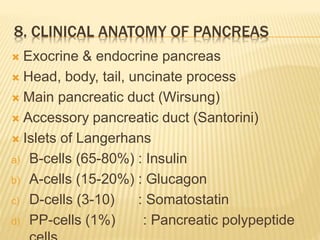
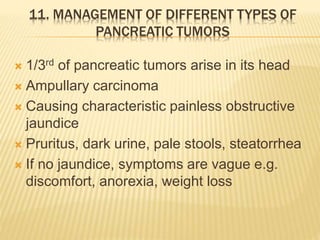
![MODEL FOR END-STAGE LIVER DISEASE (MELD)
SCORE
MELD = 3.78×ln[serum bilirubin (mg/dL)] +
11.2×ln[INR] + 9.57×ln[serum creatinine
(mg/dL)] + 6.43×aetiology(0: cholestatic or
alcoholic, 1- otherwise)
In interpreting the MELD Score in hospitalized
patients, the 3 month mortality is:
1. 40 or more — 71.3% mortality
2. 30–39 — 52.6% mortality
3. 20–29 — 19.6% mortality
4. 10–19 — 6.0% mortality
5. <9 — 1.9% mortality](https://image.slidesharecdn.com/hepaticpancreatictumors-copy-150504033539-conversion-gate01/85/Hepatic-pancreatic-tumors-28-320.jpg)



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)