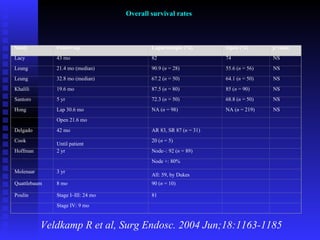
Downloaded 281 times



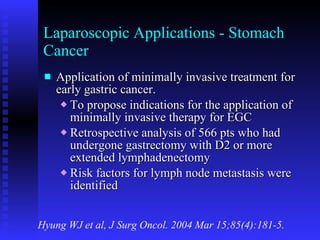
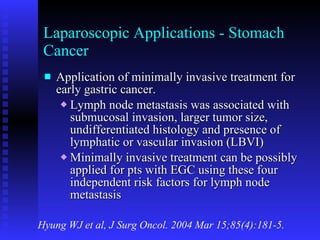

















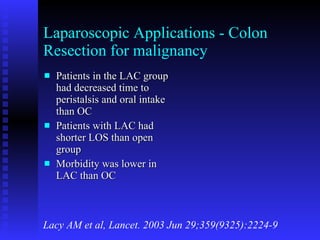
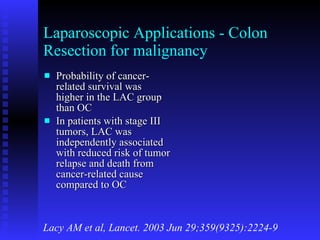
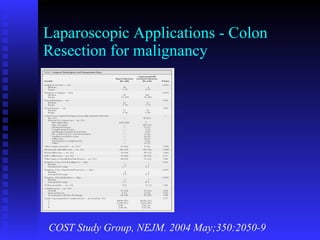






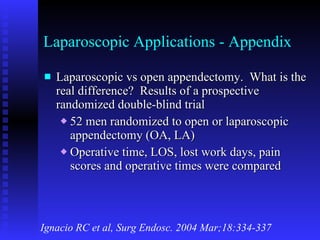
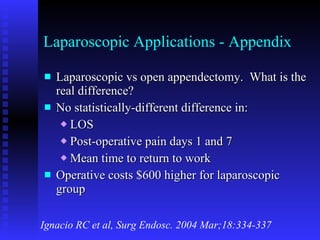
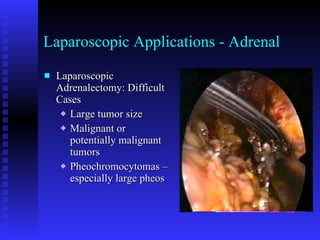
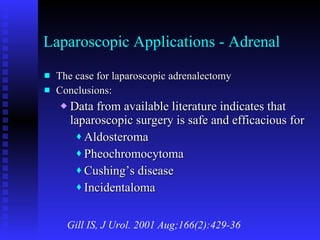
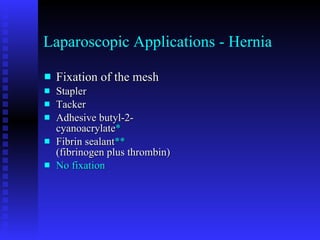
![Length of hospital stay Veldkamp R et al, Surg Endosc. 2004 Jun;18:1163-1185 Study Laparoscopic Open p value Week 5.6 ± 0.26 6.4 ± 0.23 <0.001 Hewitt 6 (57) 7 (4–9) — Milsom 6.0 (3–37) 7.0 (524) NS Delgado <70 yr 5 7 0.0001 >70 yr 6 7 0.0009 Curet 5.2 7.3 <0.05 Stage 5 (3–12) 8 (5–30) 0.01 Lacy 5.2 ± 1.2 8.1 ± 3.8 0.0012 Lezoche RHC 9.2 13.2 0.001 LHC 10.0 13.2 0.001 Bouvet 6 (2–35) 7 (4–52) <0.01 Hong 6.9 ± 5.4 10.9 ± 9.3 0.003 Koehler 8.1 (6–14) 15.3 (9–23) — Psaila 10.7 ± 4.7 17.8 ± 9.5 0.001 Khalili 7.7 ± 0.5 8.2 ± 0.2 NS Lezoche 10.5 13.3 0.027 Marubashi] 18.7 35.8 <0.0001 Franklin <50 yr 5.2 (2.0–9.2) 9.35 (517) — >50 yr 7.84 (448) 12.85 (941) Leung 6 (3–22) 8 (3–28) <0.001](https://image.slidesharecdn.com/evaluatingcurrentlaparoscopicapplicationsinsurgery-110210094633-phpapp02/85/Evaluating-Current-Laparoscopic-Applications-In-Surgery-118-320.jpg)



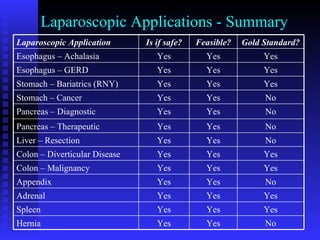

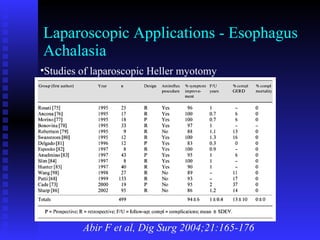
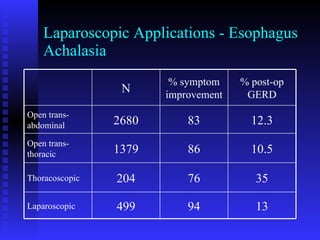
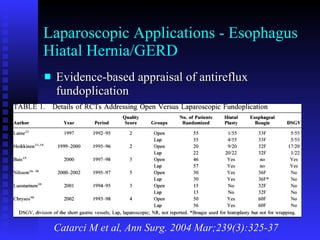
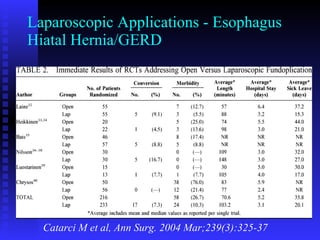
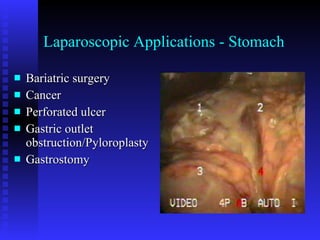
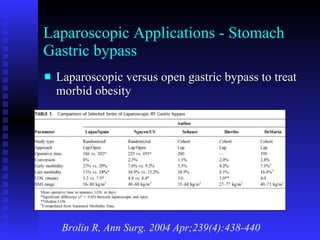
The document discusses current laparoscopic applications in various areas of surgery based on available evidence from medical literature. For the esophagus, laparoscopic Heller myotomy is established as the preferred approach for achalasia over open or thoracoscopic based on studies showing lower rates of postoperative GERD and similar symptom improvement. For hiatal hernia and GERD, laparoscopic fundoplication is the gold standard procedure based on randomized trials showing advantages over open surgery in outcomes. For gastric bypass surgery, laparoscopic approaches are preferred for treatment of morbid obesity based on cohort studies demonstrating shorter hospital stay and lower complication rates compared to open surgery. For pancreatic surgery, laparoscopic approaches are being used increasingly











































































































