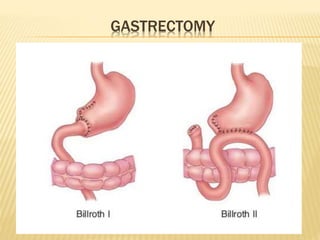
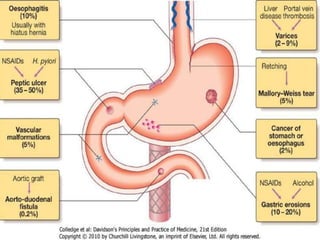
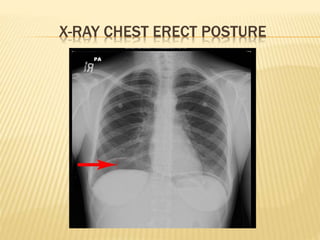
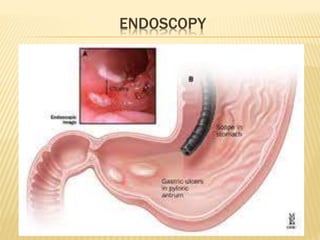
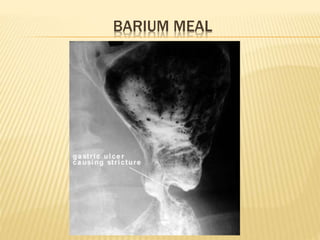
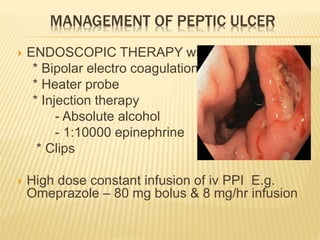
This document discusses peptic ulcer and upper gastrointestinal bleeding. It defines peptic ulcer as a lesion in the stomach or duodenum caused by gastric acid and pepsin. Risk factors include H. pylori infection, NSAID use, smoking, and stress. Clinical presentation includes epigastric pain, vomiting, weight changes, and bleeding. Investigations include endoscopy, blood tests, and imaging. Treatment involves acid suppression with PPIs, H. pylori eradication, and sometimes surgery. Upper GI bleeding refers to bleeding from the esophagus, stomach, or duodenum, with common causes being ulcers, erosions, and esophageal varices. Clinical management involves resuscitation,