Downloaded 1,029 times
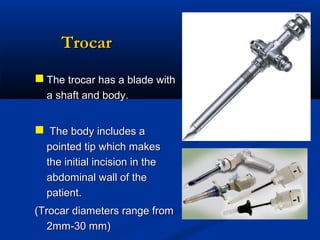
![tro-car [Fr., troisis, three +carre, side] noun
a sharp-pointed surgical instrument
fitted with a cannula and used
especially to insert the cannula into
a body cavity
cannula - [L., dim of
canna,reed] noun
a tube that is inserted into a cavity
by means of a trocar filling it’s lumen](https://image.slidesharecdn.com/sreejoylapfuture-131216212417-phpapp02/85/LAPAROSCOPIC-SURGERY-PAST-PRESENT-AND-FUTURE-44-320.jpg)

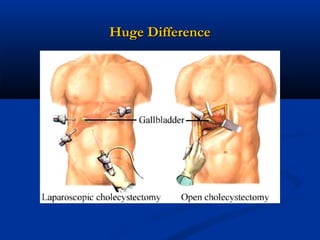









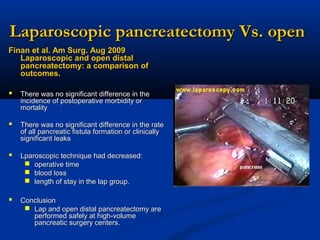







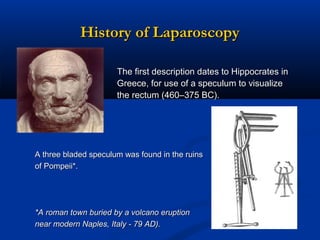
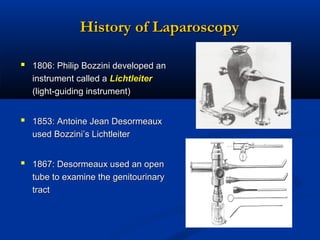
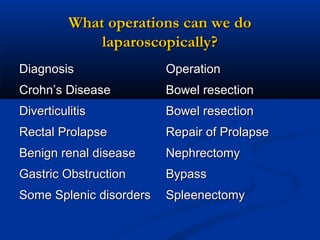
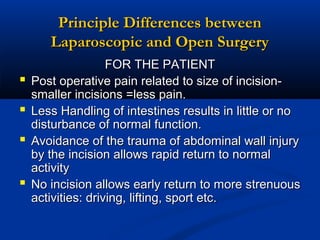
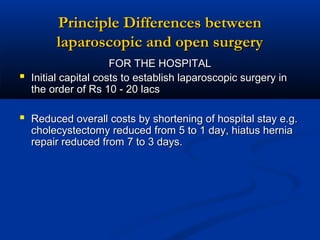
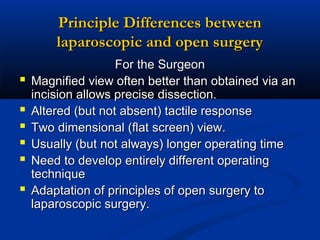
The document provides a comprehensive history of laparoscopy, tracing its evolution from ancient descriptions to modern techniques, highlighting key milestones and innovations by various medical pioneers. It discusses the advantages of laparoscopic surgery over traditional open surgery, emphasizing reduced postoperative pain, faster recovery, and lower hospital costs. Additionally, it outlines common laparoscopic procedures and the necessary instruments and techniques involved in the process.











































































































