
Downloaded 50 times

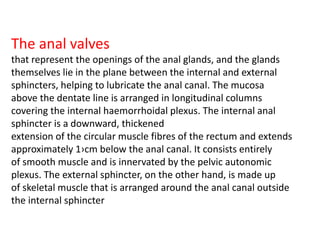



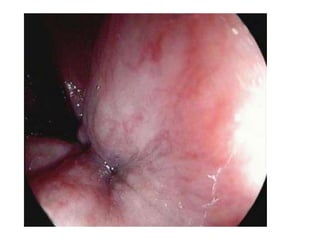
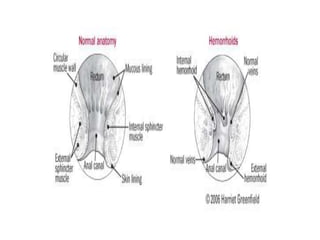
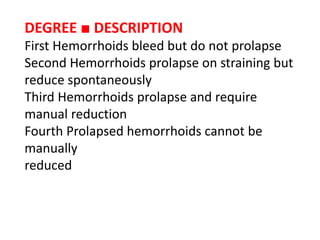
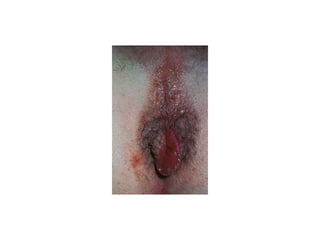
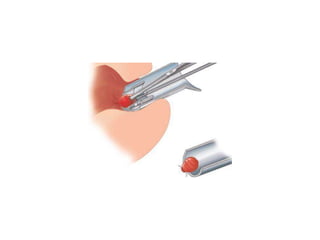



This document provides information on haemorrhoids (also known as hemorrhoids), including: - Anatomy of the anal canal and haemorrhoidal tissue - Epidemiology of symptomatic haemorrhoids, affecting around 4.4% of the global population - Common causes like straining, pregnancy, obesity, and familial tendency - Grading of internal haemorrhoids from first to fourth degree based on degree of prolapse - Treatment options like rubber band ligation, sclerotherapy, excisional or stapled haemorrhoidectomy depending on severity


















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















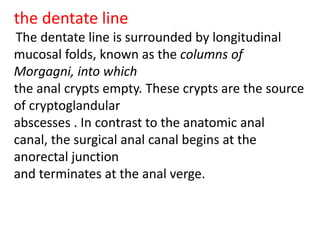
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)