Downloaded 1,028 times



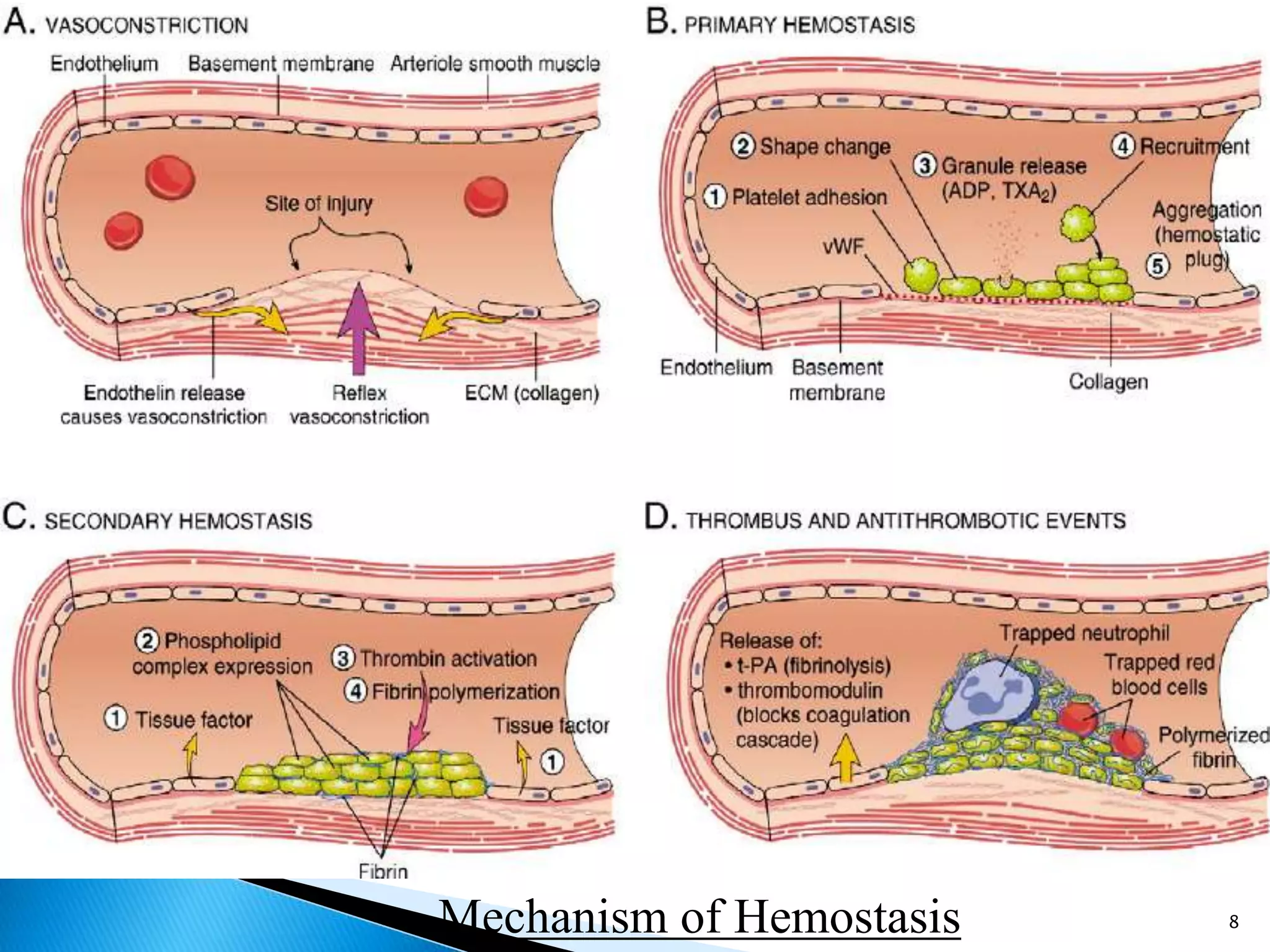

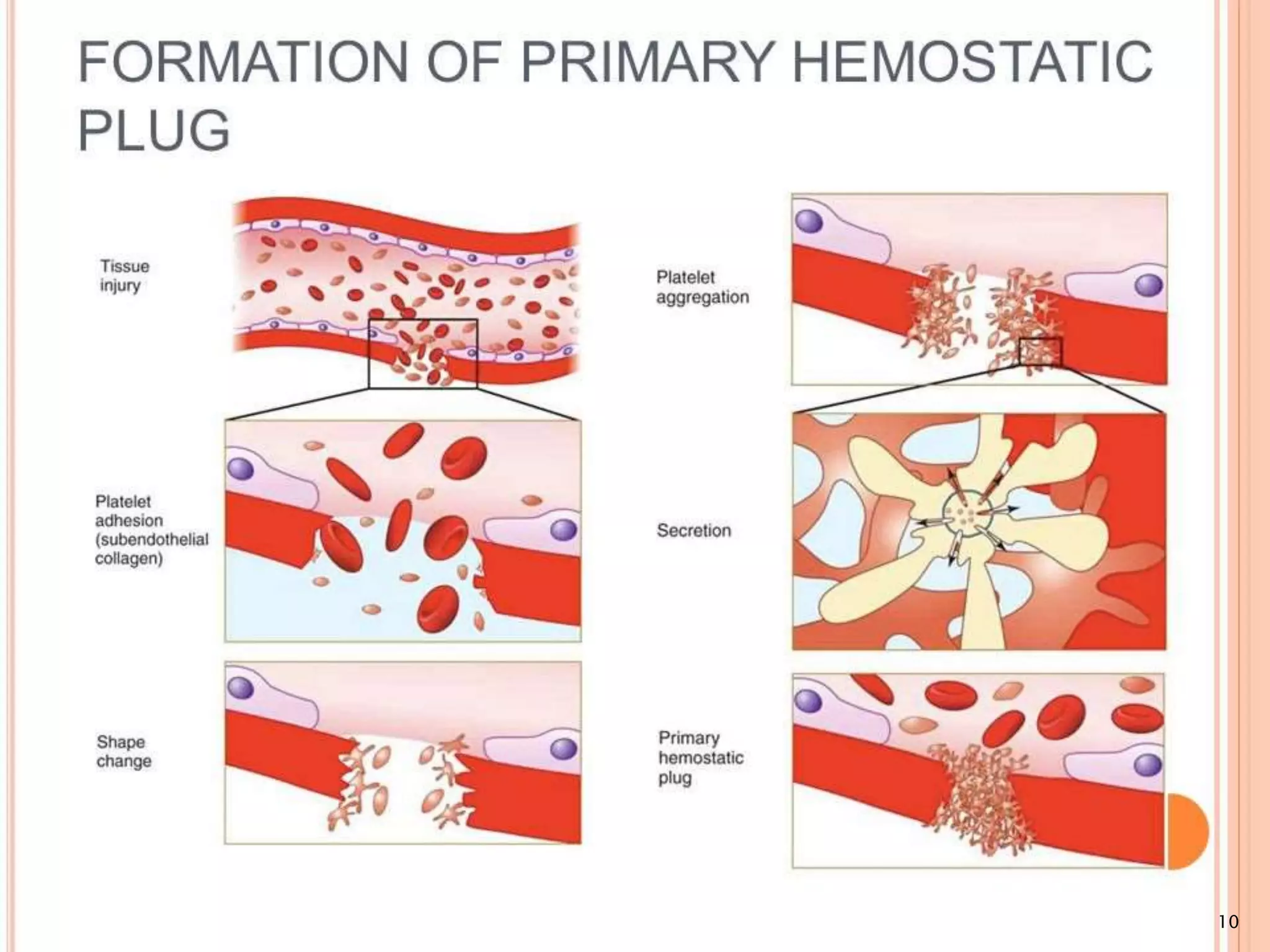























The document discusses hemorrhage, its classification, etiologies, and management techniques. It details various types of hemorrhage based on source, nature, time, volume, speed, and blood loss percentage, as well as the mechanisms of hemostasis. Furthermore, it outlines clinical evaluation procedures, laboratory tests for assessing bleeding risk, and mechanical, chemical, and thermal methods for achieving hemostasis.





























































































