Downloaded 207 times

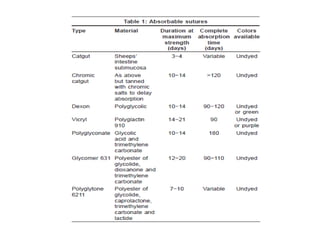


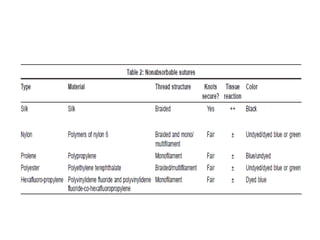

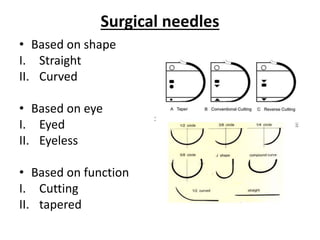
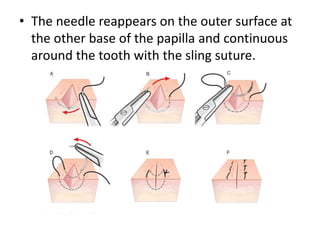
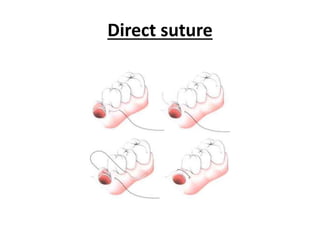
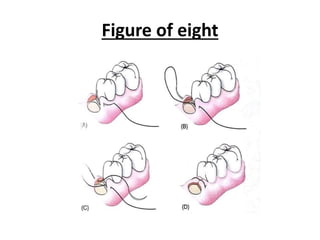
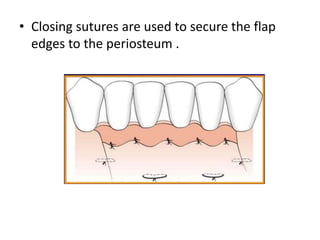

This document discusses suturing materials and techniques used in dentistry. It begins with an introduction to sutures and their purpose in closing wounds. It then covers general suturing principles, features of ideal suture materials, sizes of sutures, classifications of suture materials including absorbable and non-absorbable types. The document also discusses surgical needles, knots, and various suturing techniques including interrupted, continuous, mattress, and sling sutures. It emphasizes selecting the appropriate suture size and material for the wound and tissue being closed. In conclusion, it states that knowledge of suturing is important for surgical procedures and innovation in materials can decrease infections.














































































