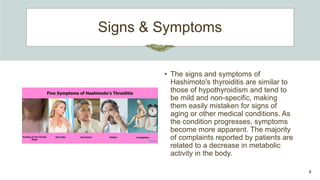
Hashimoto's thyroiditis is an autoimmune disease characterized by the body's immune system attacking the thyroid gland, causing inflammation. It is the leading cause of hypothyroidism in the United States, occurring more often in women than men, possibly due to hormonal factors. Symptoms are generally mild but include fatigue, weight gain, dry skin and hair, and constipation. The condition is diagnosed through blood tests showing low thyroid hormone and high thyroid stimulating hormone levels. While there is no cure, symptoms can be managed through lifelong thyroid hormone replacement medication.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

