Download as PDF, PPTX









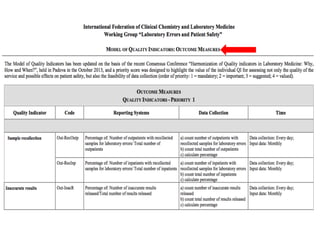
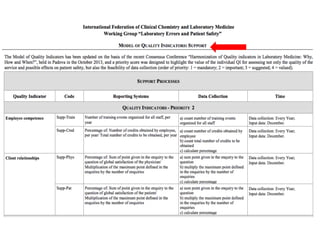




The document discusses harmonization of quality indicators (QIs) in medical laboratories. It notes that while QIs are important for quality improvement, there is currently no consensus on common QIs or how they should be defined and measured. The Working Group on Laboratory Errors and Patient Safety has developed a Model Quality Indicator (MQI) to address this issue, which defines 53 measurements across 27 QIs. Laboratories can now report results to the MQI website voluntarily. Statistical analysis of early participation in the MQI shows the most widely used QIs relate to pre-analytical errors, analytical test performance, and post-analytical issues. However, broader adoption remains a challenge.









































































































