








![INTERNAL QUALITY CONTROL
• Patient Data as Alternate Quality Control-
- Correlation of test results Across patients-
- Trends in patient results
- Average of Normal
- Correlation of test results within same patient
- With clinical findings eg- ammonia levels
with altered sensorium
- With Other tests eg- BUN & creatinine
- With same test but alternate method eg-
Infectious Serology, Tumour markers
- Delta check- Reference Change Value (RCV) for
chemistry & immunoassay analytes based on
equation: RCV = 2½ × Z × [CVA
2 + CVI
2]½ where
Z=1.96, CVA is Analytical variance ,
CVI is intra-individual biological variance](https://image.slidesharecdn.com/qualitycontrolinclinicallaboratory-190217115231/75/Quality-Control-In-Clinical-Laboratory-13-2048.jpg)














The document outlines quality control processes in clinical laboratories, emphasizing the importance of adhering to quality management standards such as ISO 15189. It discusses the consequences of poor quality, the objectives of quality management, various quality control measures, and the implementation of total quality management frameworks in laboratory settings. Additionally, it highlights proficiency testing, error detection, and the significance of maintaining high standards to ensure accurate and reliable laboratory results.
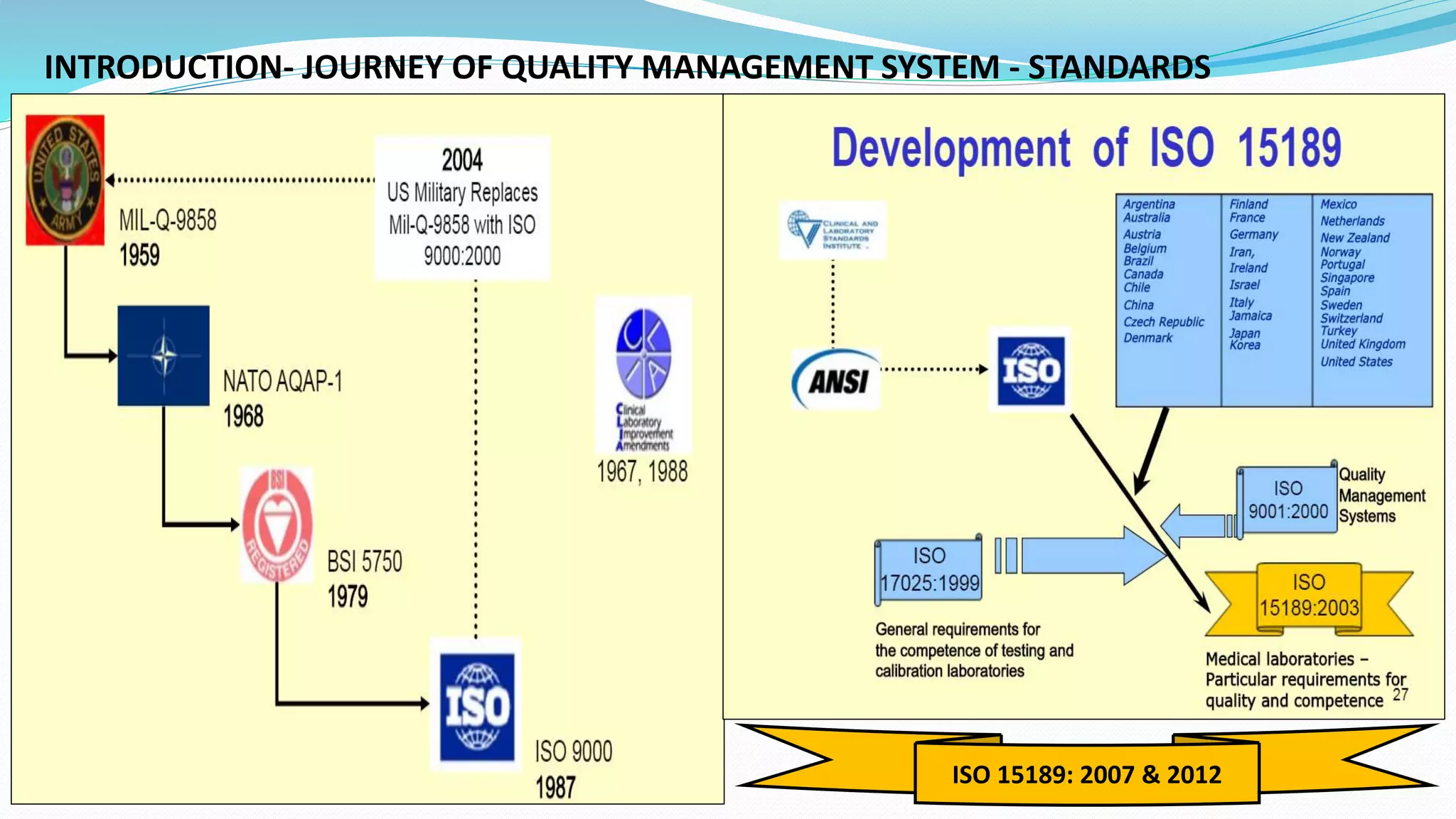
Overview of Quality Control in clinical labs, the journey and standards, emphasizing ISO 15189.
Discusses the need for quality in individual labs, risks of poor quality, and objectives to ensure high healthcare standards.
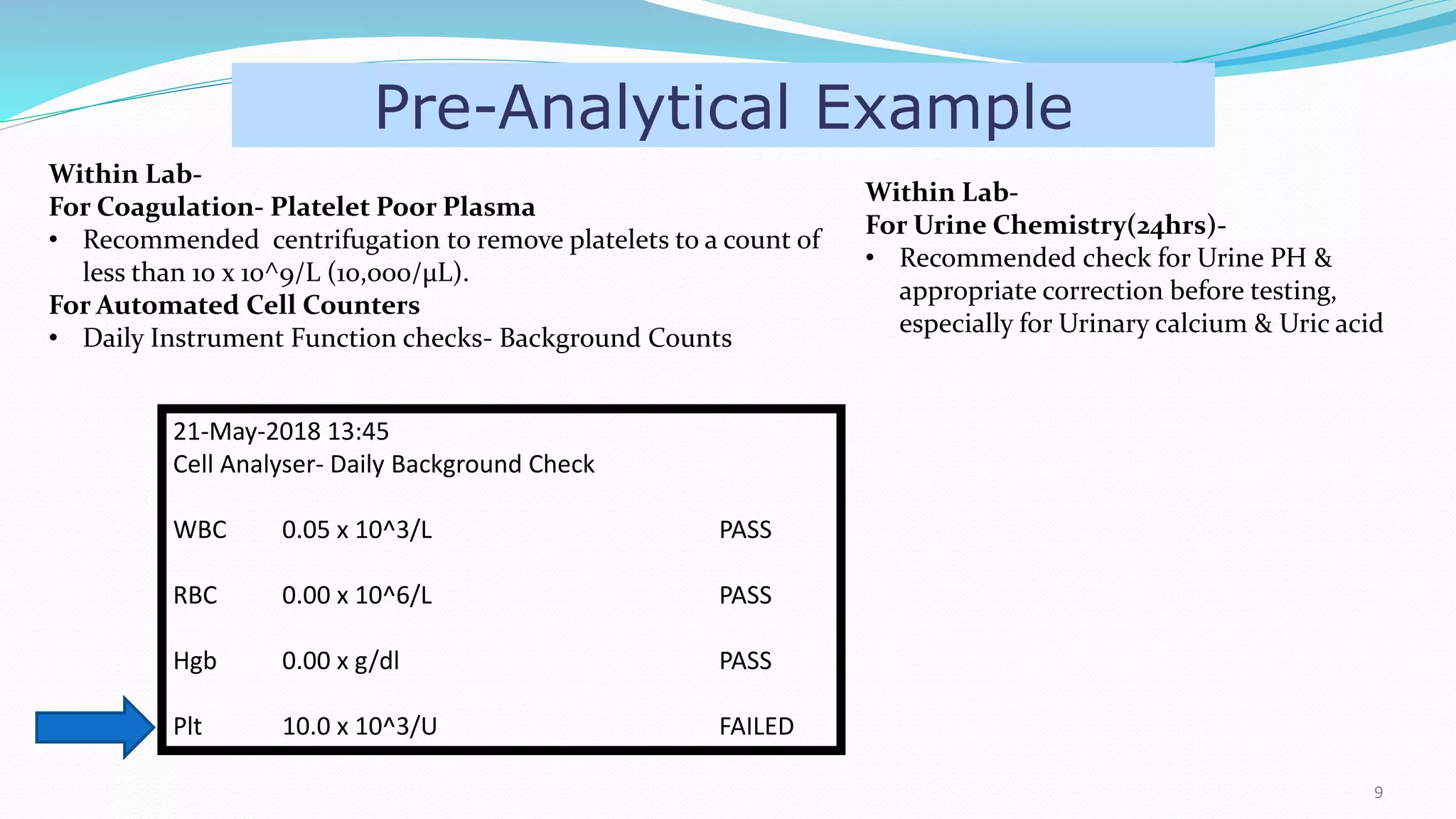
Focused on laboratory errors, best practices for sample collection, including anticoagulant considerations and pre-analytical variables.
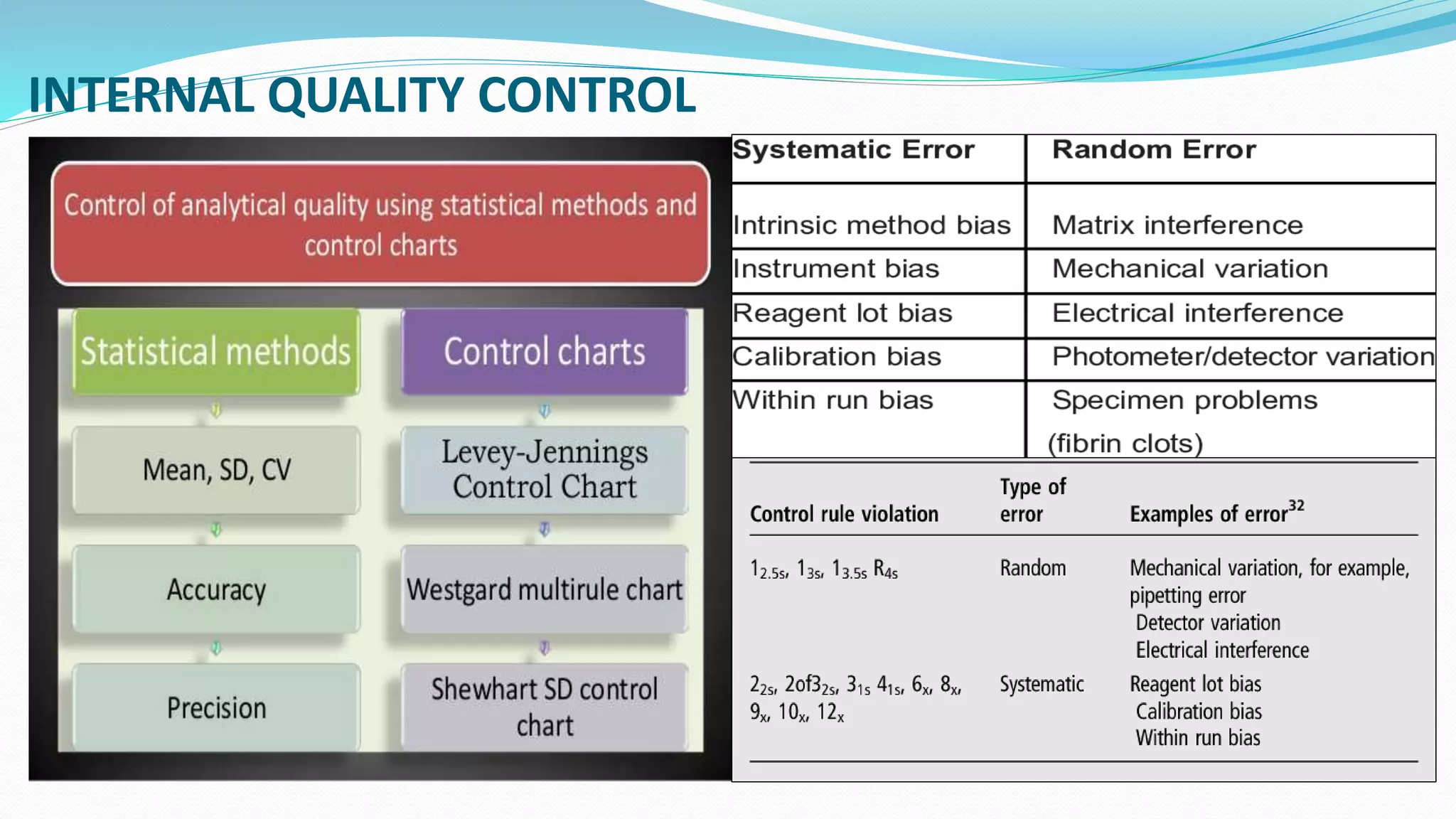
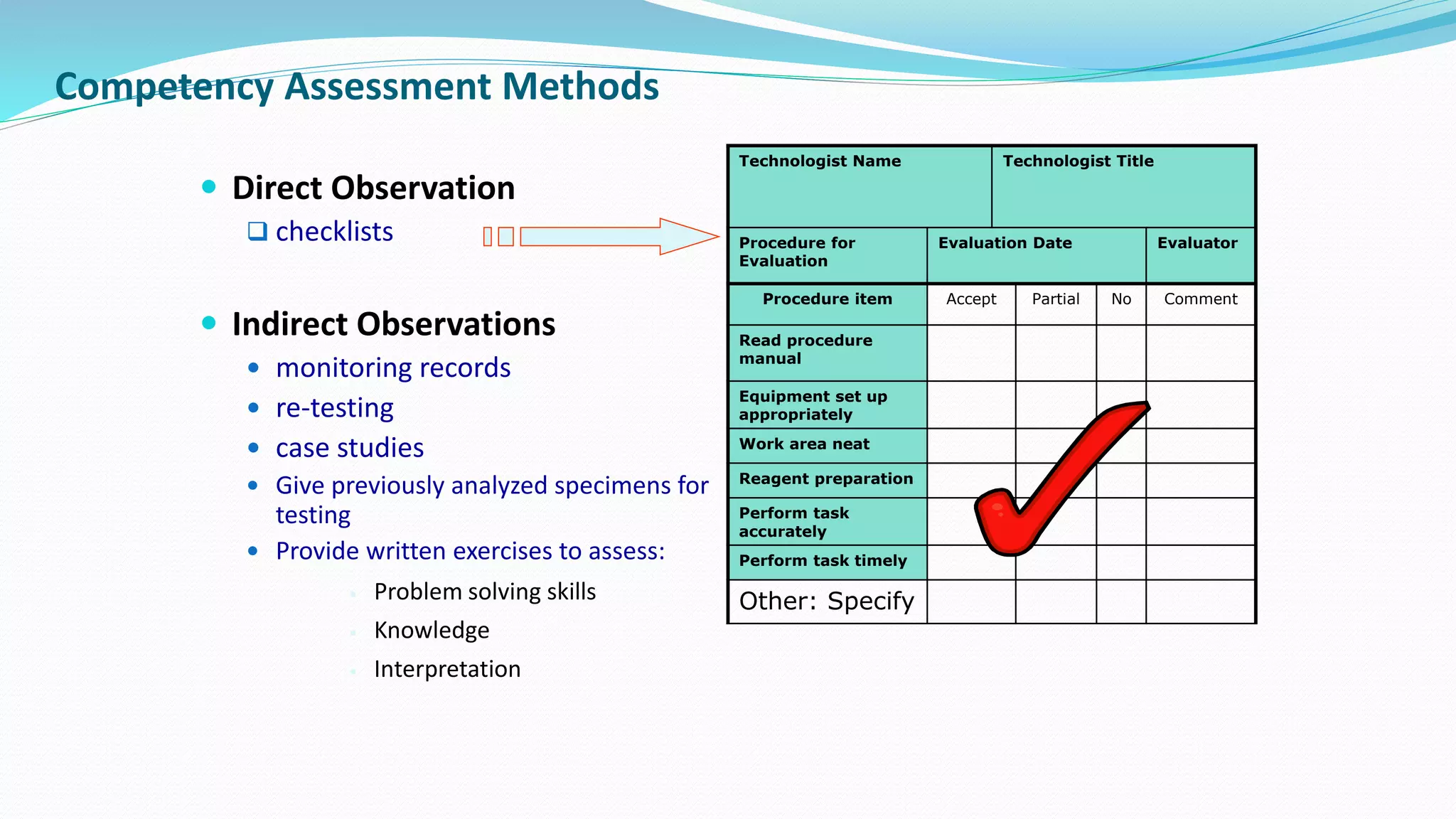
Internal Quality Control methods for sample testing including calibration, control materials, and tracking test results.
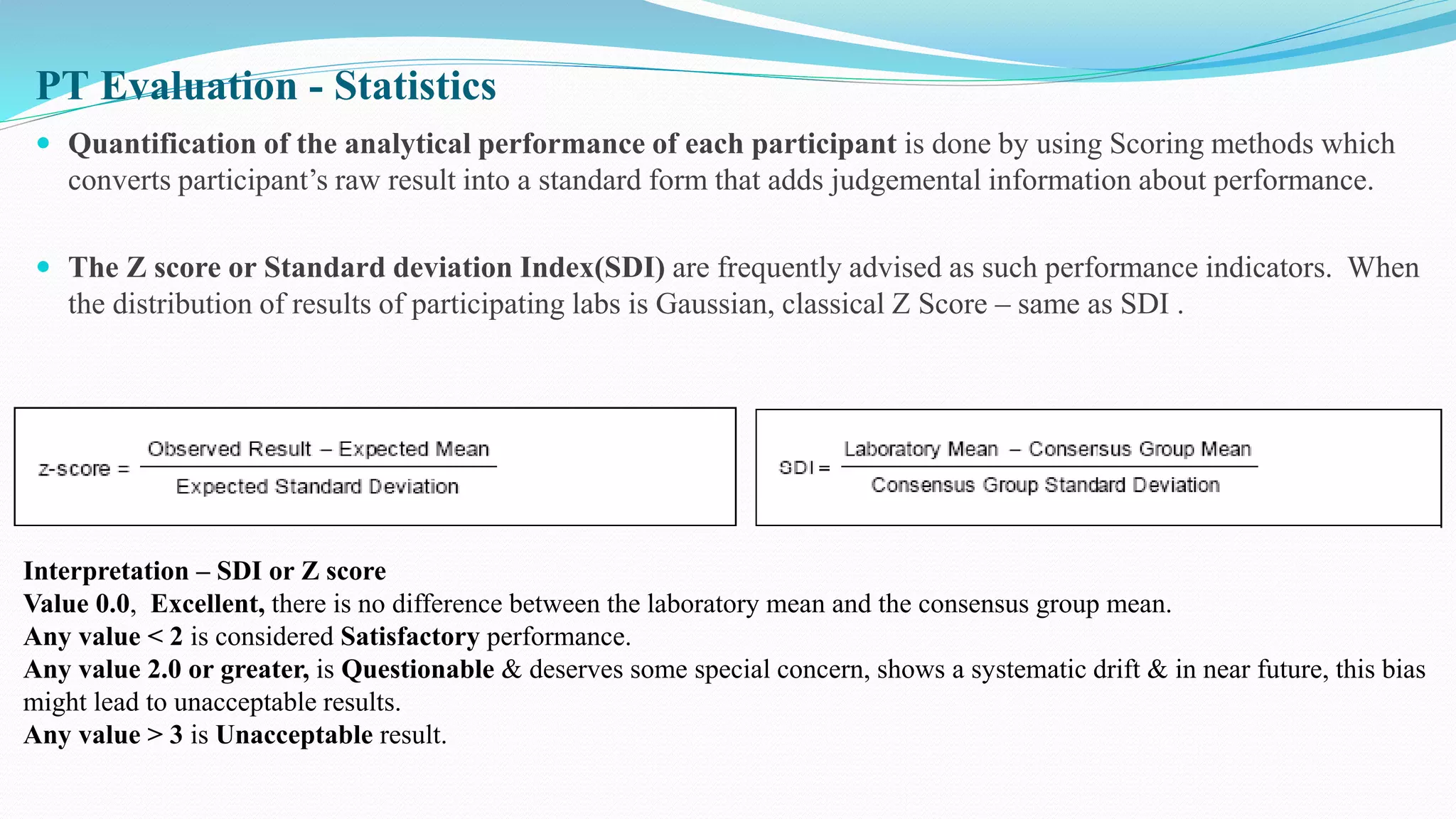
Selection and standards for External Quality Control Programs; evaluation of proficiency testing results.
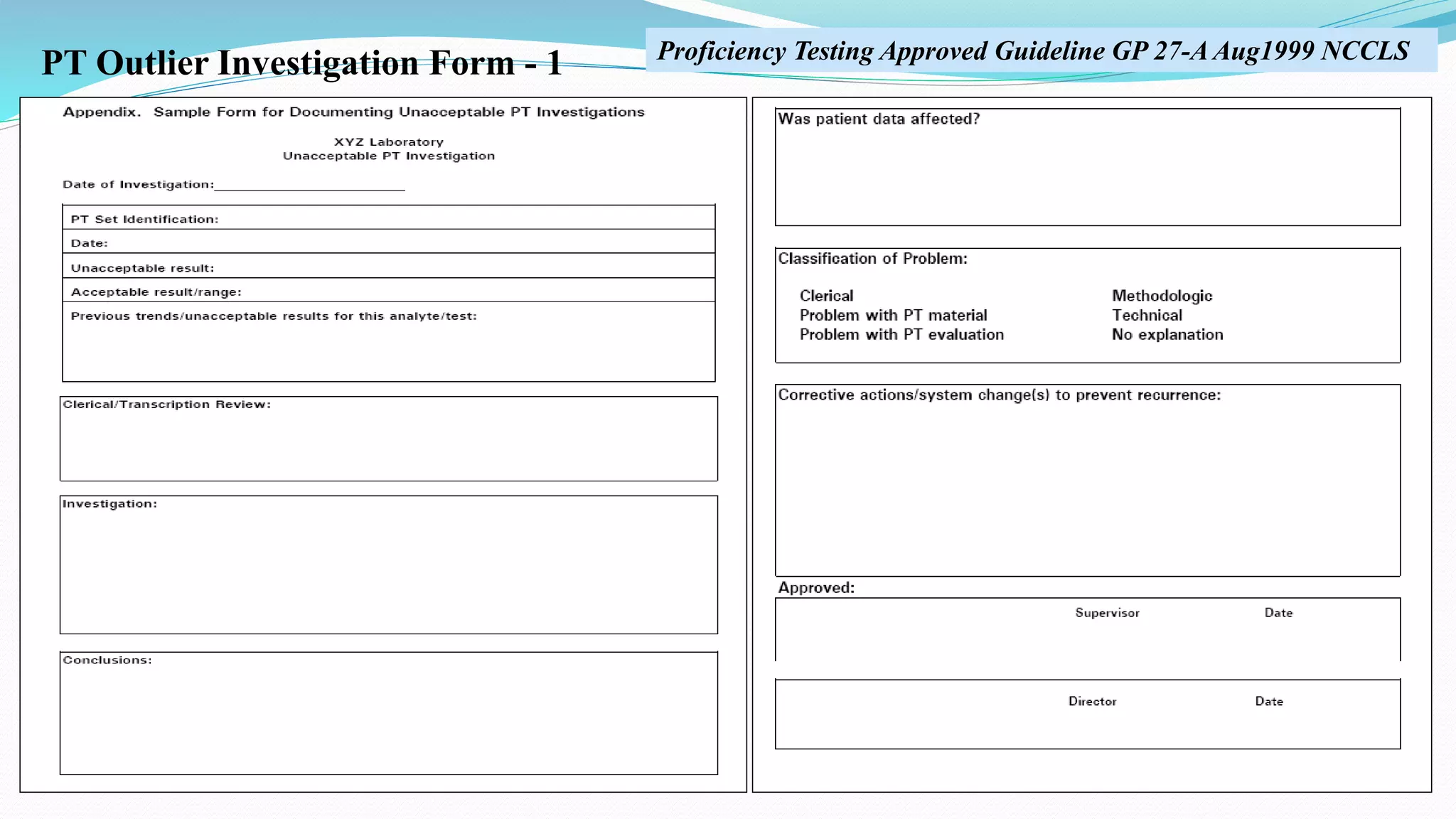
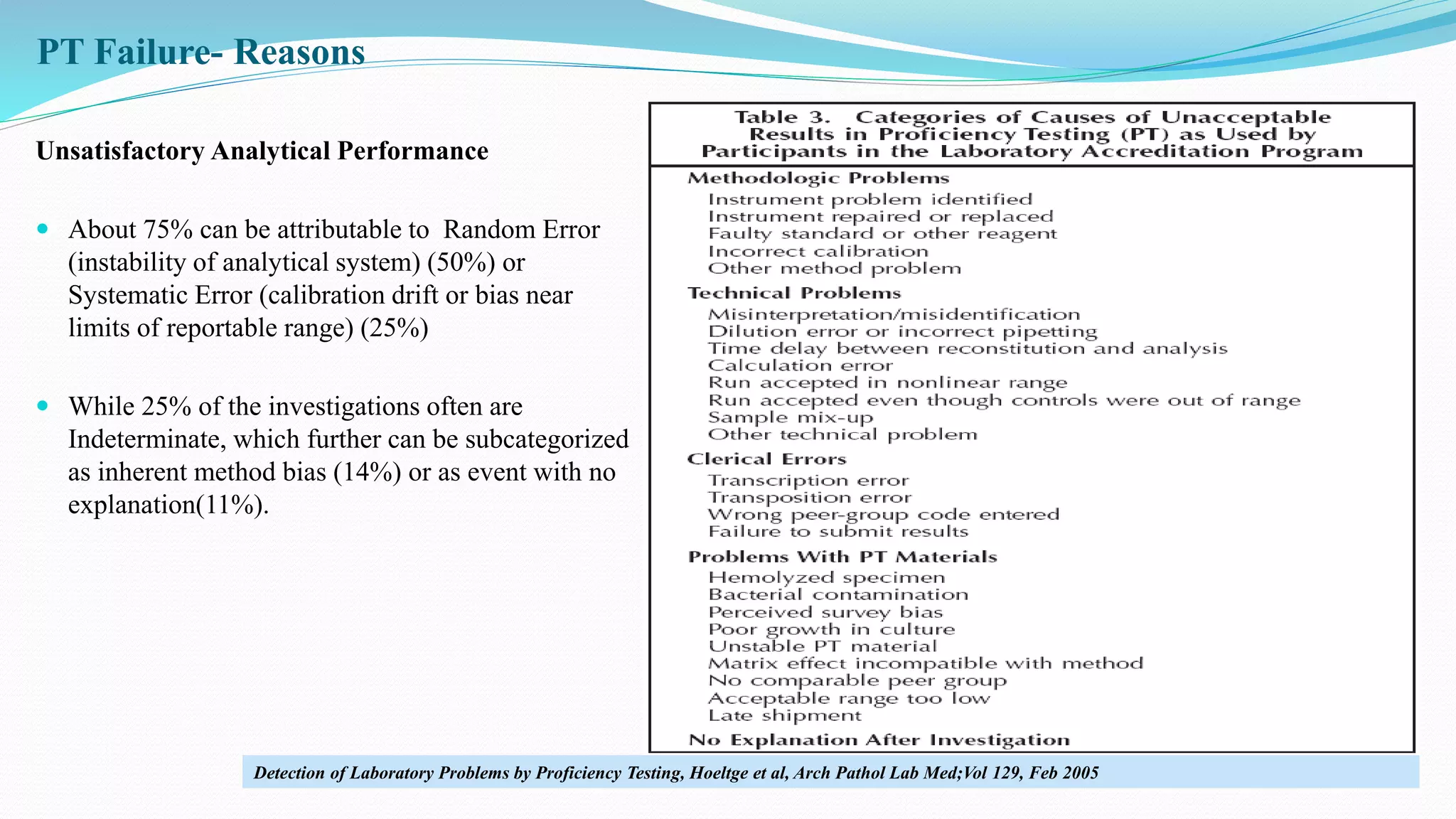
Approaches to analyze proficiency testing failures and investigation forms to trace issues in laboratory performance.
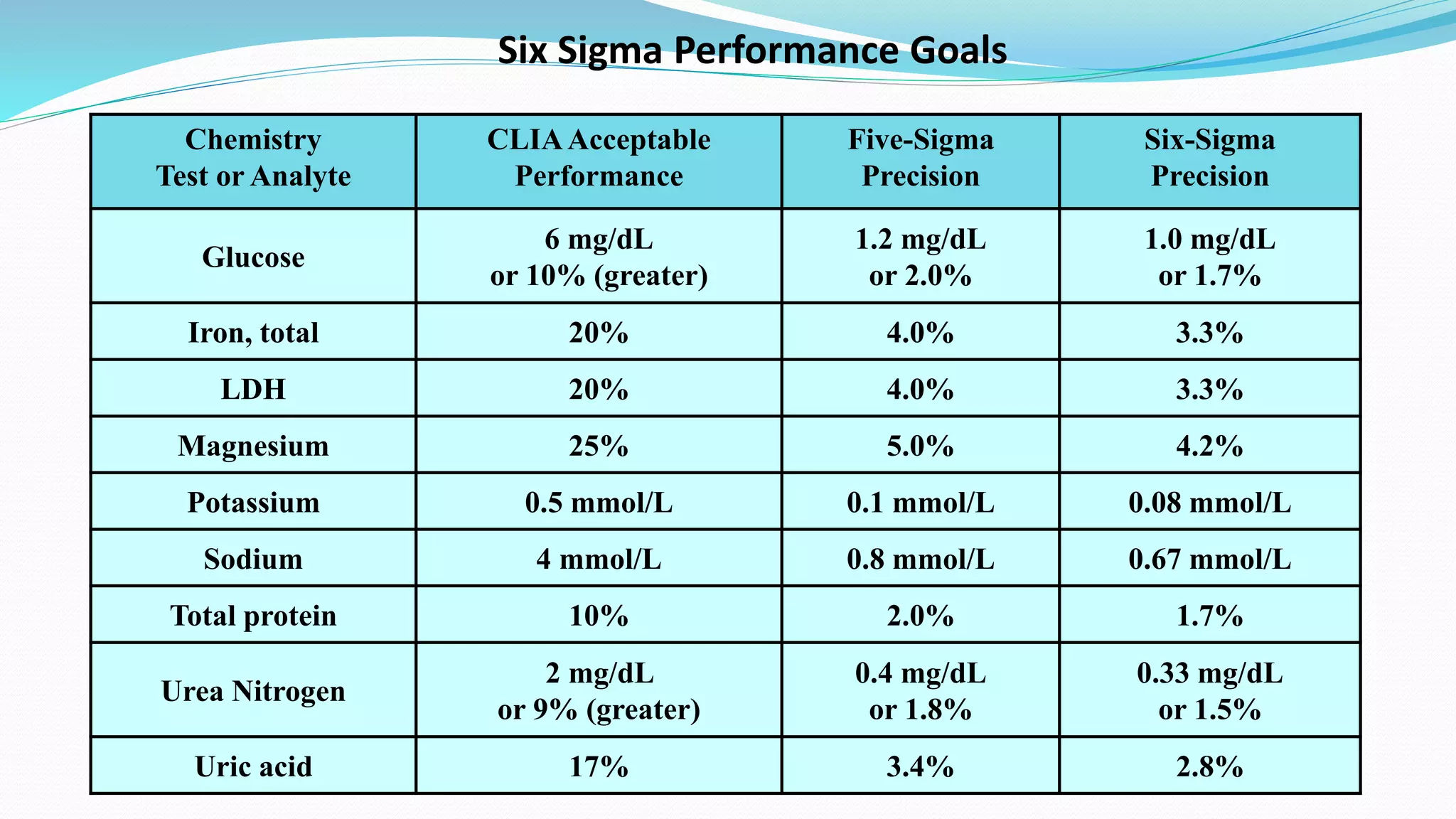
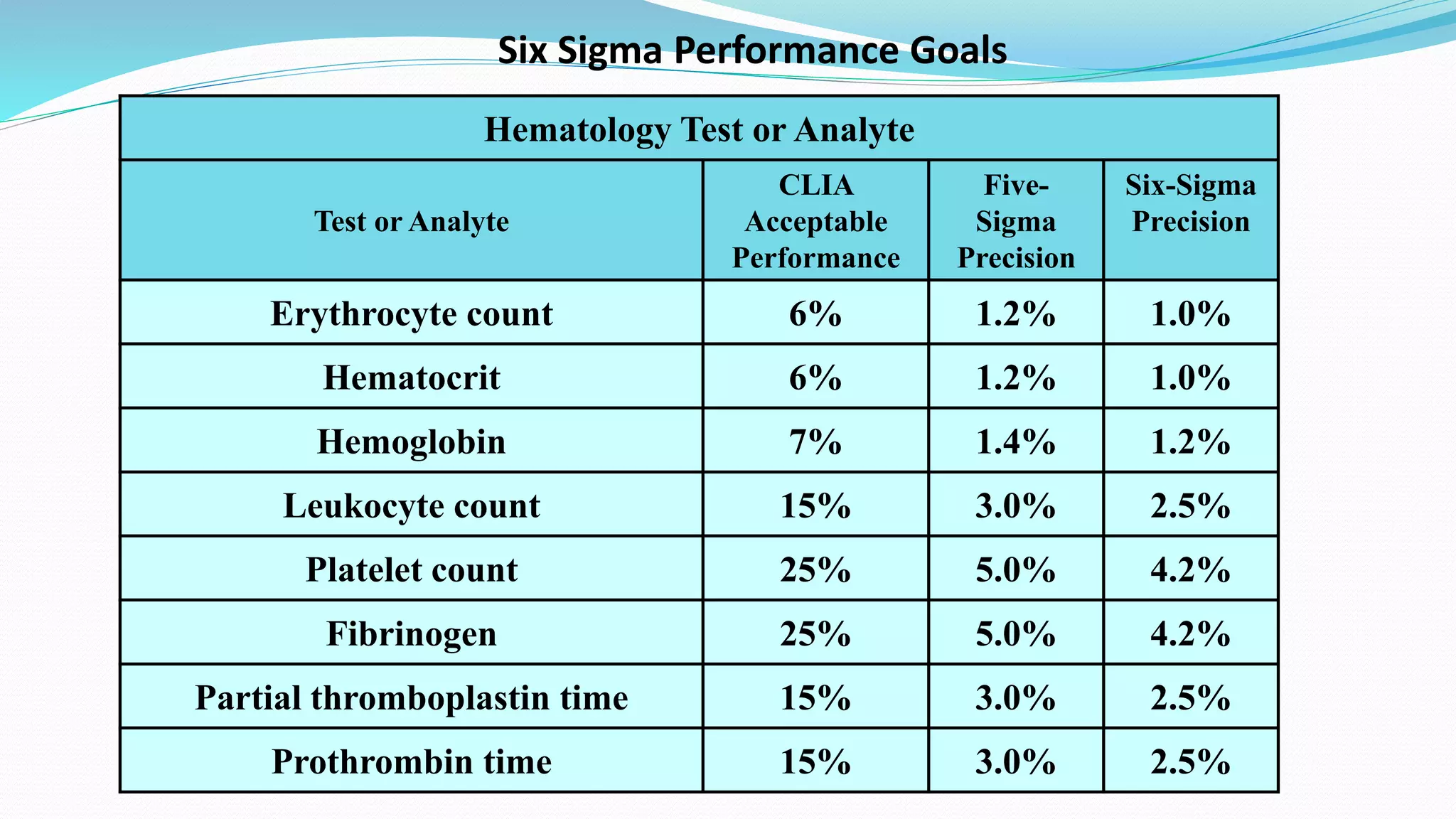
Implementation of Six Sigma methodology to enhance analytical performance and reduce errors in laboratory testing.
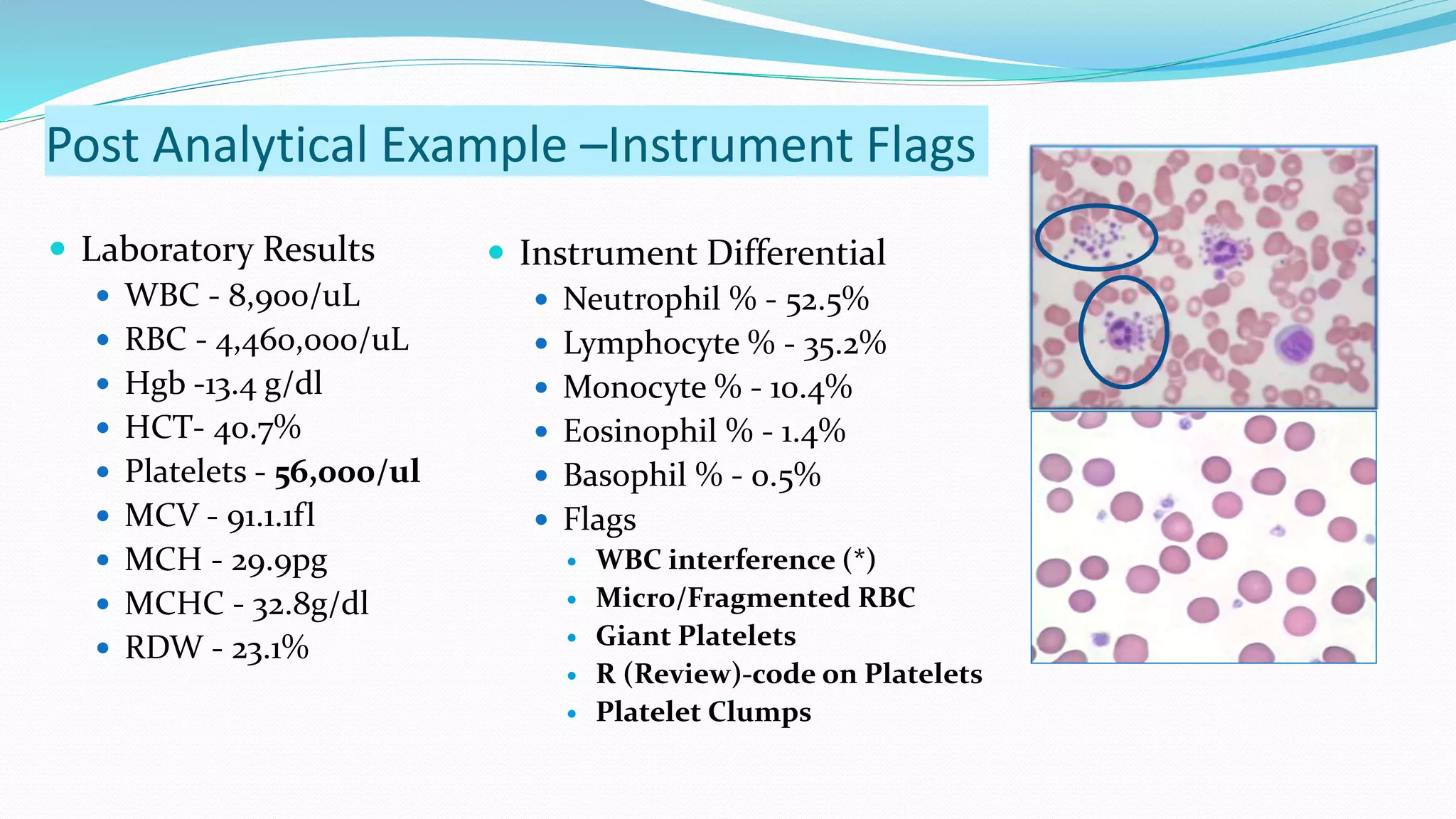
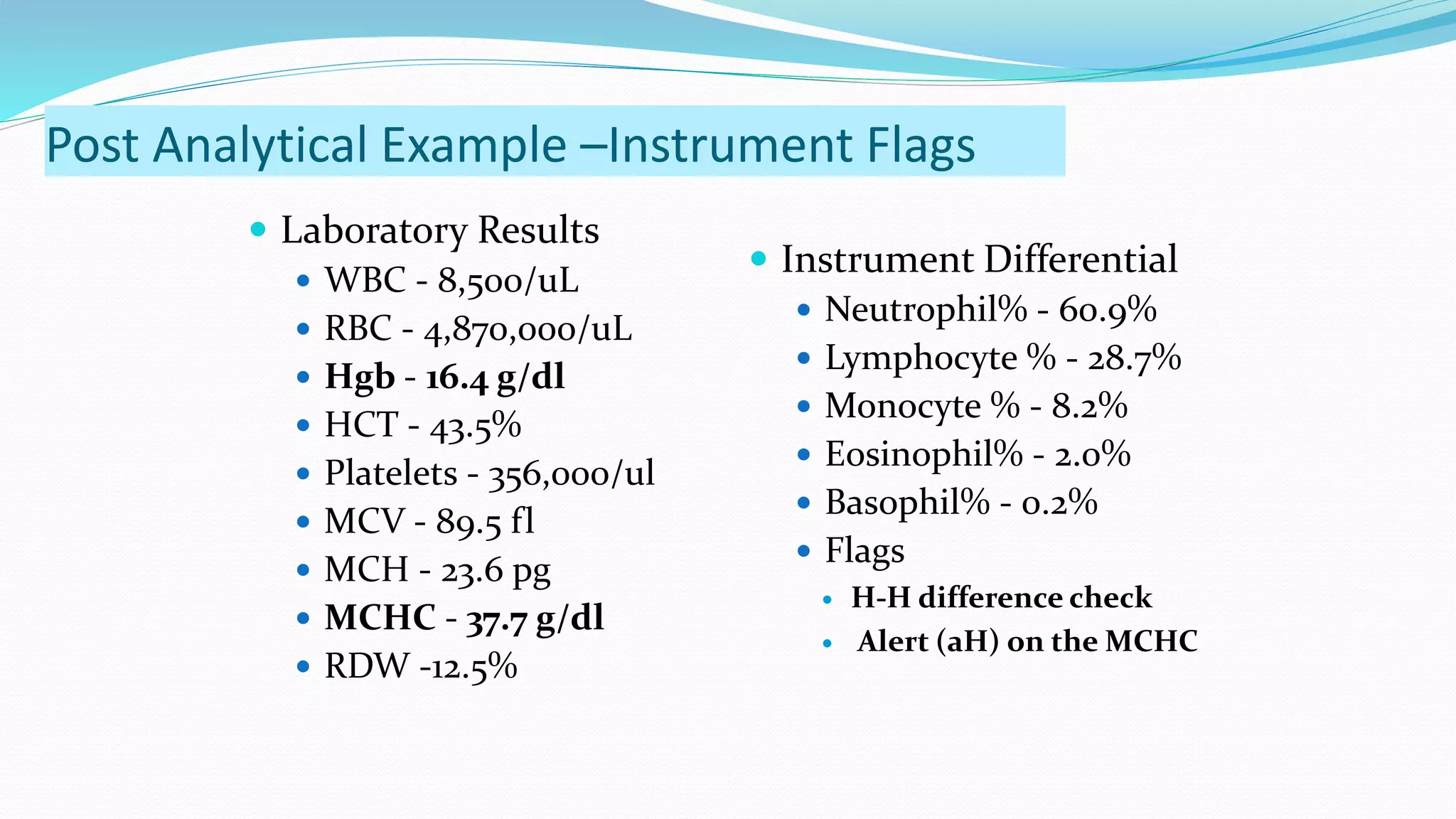
Extension of the reporting process after analysis including instrument flags and prompt reporting of results.
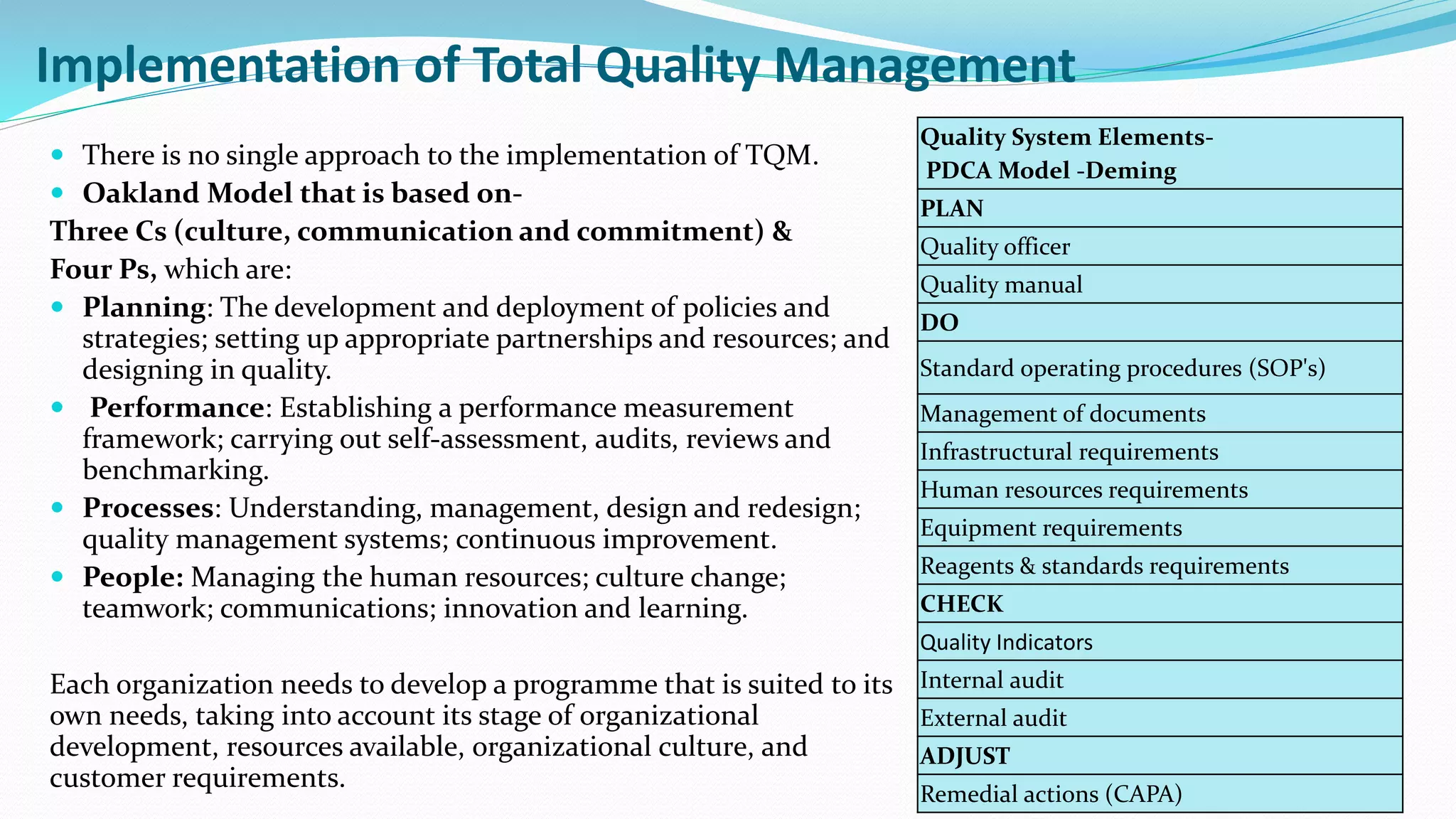
Strategies for establishing Total Quality Management in labs emphasizing a systematic approach to quality.
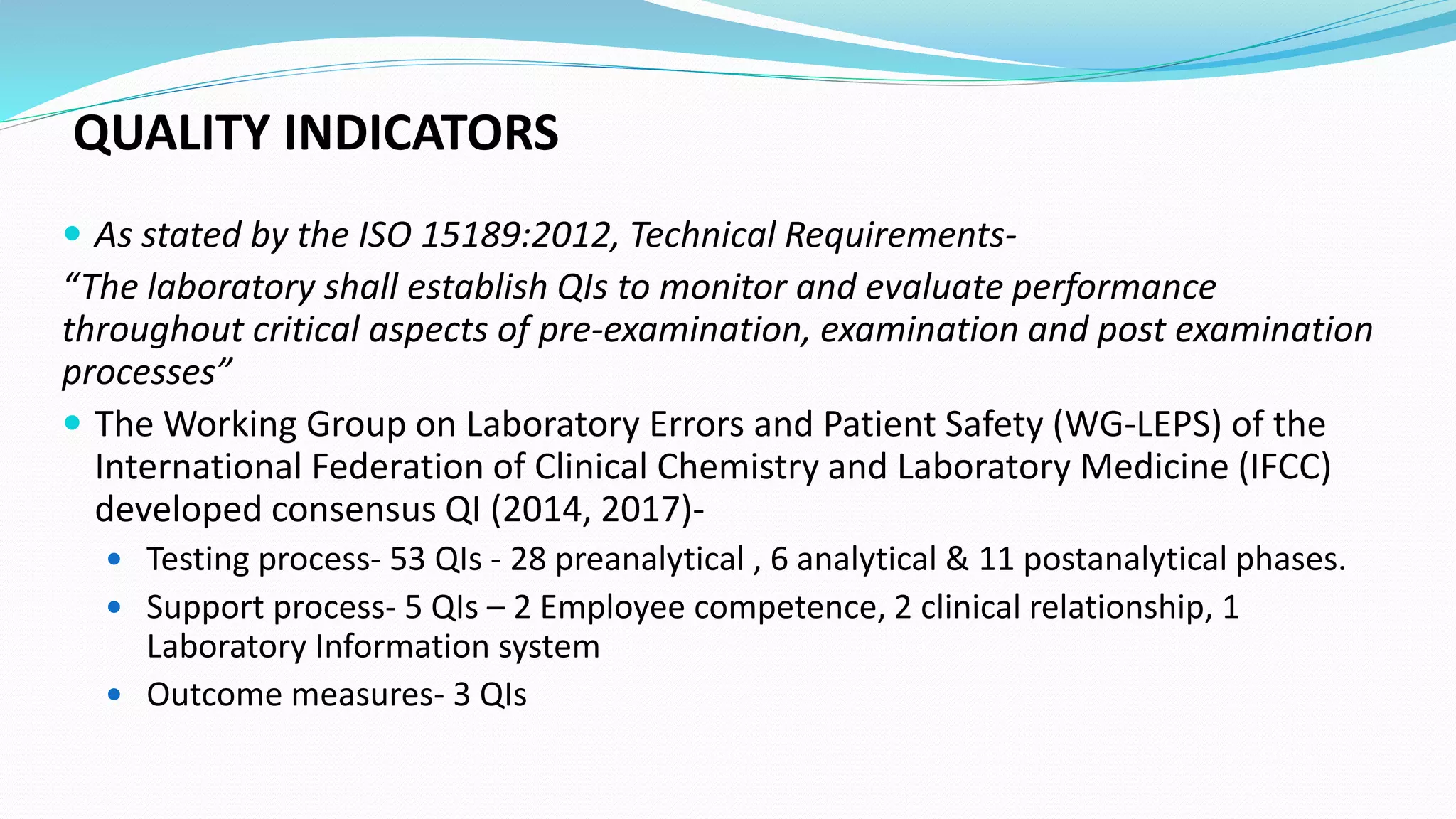
Establishment of quality indicators as per ISO requirements and benchmarks for laboratory performance.









































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)













