Downloaded 69 times

![DEFINITIONS
Gingival recession is the apical shift of the marginal gingiva from its normal
position on the crown of the tooth to levels on the root surface beyond the
cemento enamel junction
[Loe H-1992].
• Gingival recession is defined as “the displacement of marginal gingiva
apical to the cemento-enamel junction (CEJ).” (American Academy of
Periodontology 1992)](https://image.slidesharecdn.com/gingivalrecessionaries-210420070002/75/Gingival-recession-aries-4-2048.jpg)
![• The term “marginal tissue recession” is considered to be more accurate than
“gingival recession,” since the marginal tissue may have been alveolar
mucosa.
• Marginal tissue recession is defined as the displacement of the soft tissue
margin apical to the cemento-enamel junction (CEJ)
(American Academy of Periodontology 1996)
• Gingival recession is defined as the apical migration of the junctional
epithelium with exposure of root surfaces.
[Kassab MM, Cohen RE-2003].](https://image.slidesharecdn.com/gingivalrecessionaries-210420070002/75/Gingival-recession-aries-5-2048.jpg)





































































































































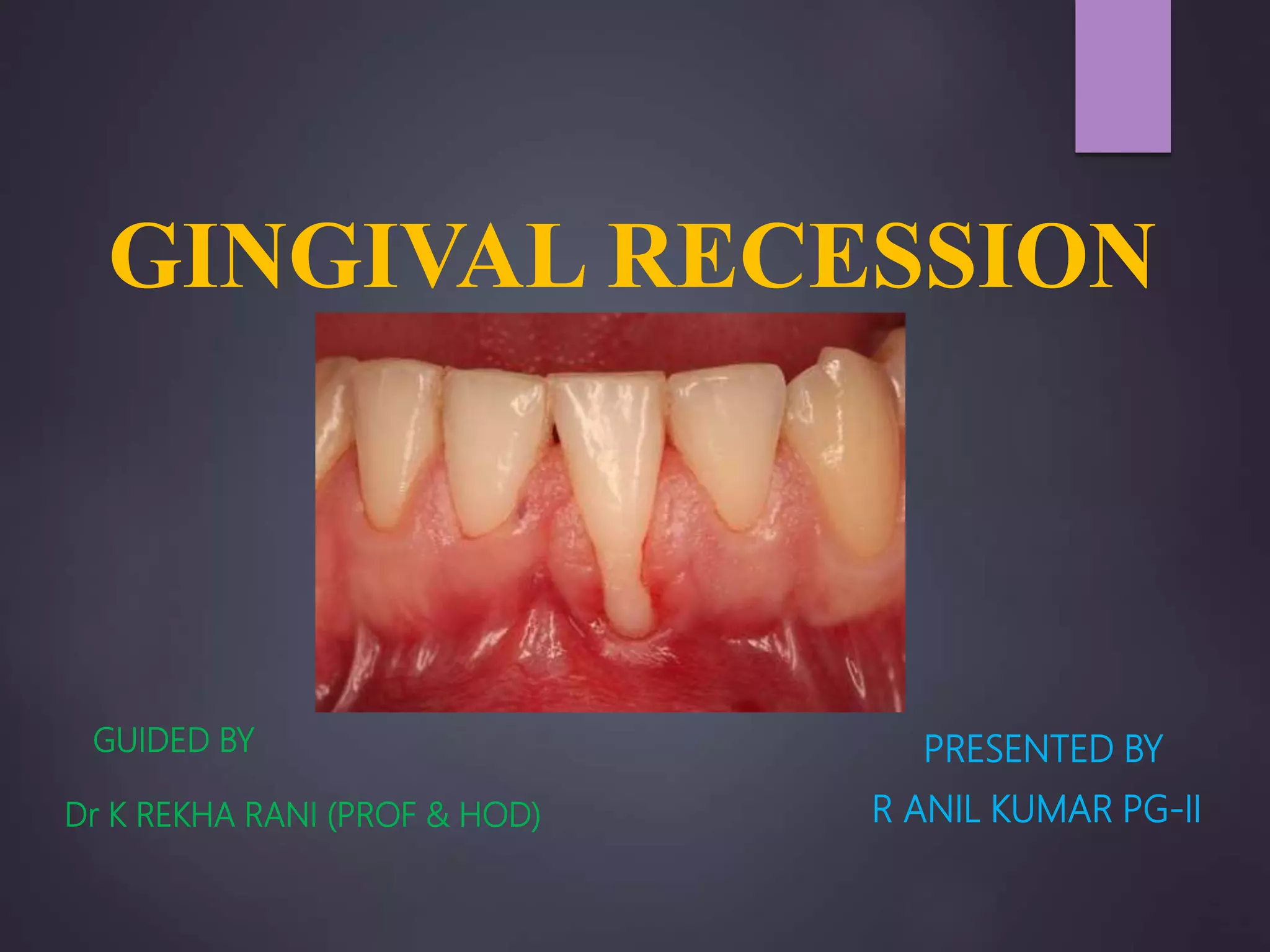
The document discusses gingival recession, characterized by the apical movement of the gingival margin from the cemento-enamel junction, along with its definitions, classifications, etiology, prognosis, and treatment techniques. Various classification systems for gingival recession are highlighted, detailing the limitations and proposed modifications aimed at improving diagnosis and treatment outcomes. Treatment options range from non-surgical to surgical methods, emphasizing the importance of factors such as the degree of recession and the condition of nearby tissues.
















































![PERIODONTAL WOUND HEALING [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/periodontalwoundhealingautosaved-240205115031-ce7a6d10-thumbnail.jpg?width=640&height=640&fit=bounds)
![Periodontal Treatment of Medically Compromised Patients [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/periodontaltreatmentofmedicallycompromisedpatientsautosaved-240205114527-6e5affd6-thumbnail.jpg?width=640&height=640&fit=bounds)




























