Downloaded 46 times


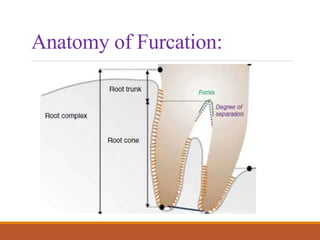









This document discusses furcation involvement and its treatment. It defines furcation as the area of division between roots in multi-rooted teeth. Furcation involvement occurs when periodontal disease invades this area. Factors that can lead to furcation involvement include long-term plaque, local anatomy like root length and shape, and trauma. Furcation involvement is classified using systems like Glickman or Tarnow & Fletcher based on severity and depth of invasion. Treatment depends on the grade of involvement and may include non-surgical approaches like scaling and root planing or surgical options like root resection, hemisection, or bicuspidization to eliminate furcation involvement.










































































