Downloaded 53 times
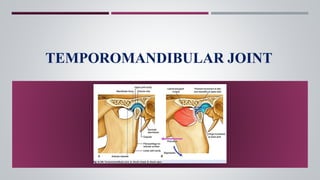

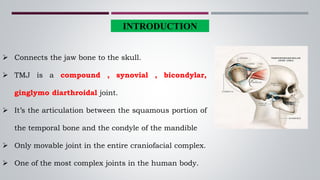








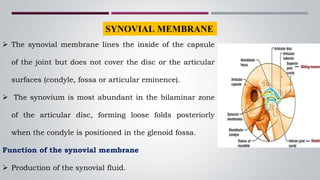

































The temporomandibular joint (TMJ) connects the jaw bone to the skull. It is a complex synovial joint that allows for movement of the mandible during chewing and talking. The TMJ has both bony and soft tissue components including the condyle, glenoid fossa, articular disc, joint capsule, ligaments and muscles. The TMJ develops late in utero and has a complex anatomy that facilitates its range of motion. Disorders can affect the TMJ resulting in problems like pain, limited movement or locking of the jaw.































![Temporomandibular joint [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/temporomandibularjointautosaved-230521065437-1cbd4148-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERIODONTAL WOUND HEALING [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/periodontalwoundhealingautosaved-240205115031-ce7a6d10-thumbnail.jpg?width=640&height=640&fit=bounds)
![Periodontal Treatment of Medically Compromised Patients [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/periodontaltreatmentofmedicallycompromisedpatientsautosaved-240205114527-6e5affd6-thumbnail.jpg?width=640&height=640&fit=bounds)




























