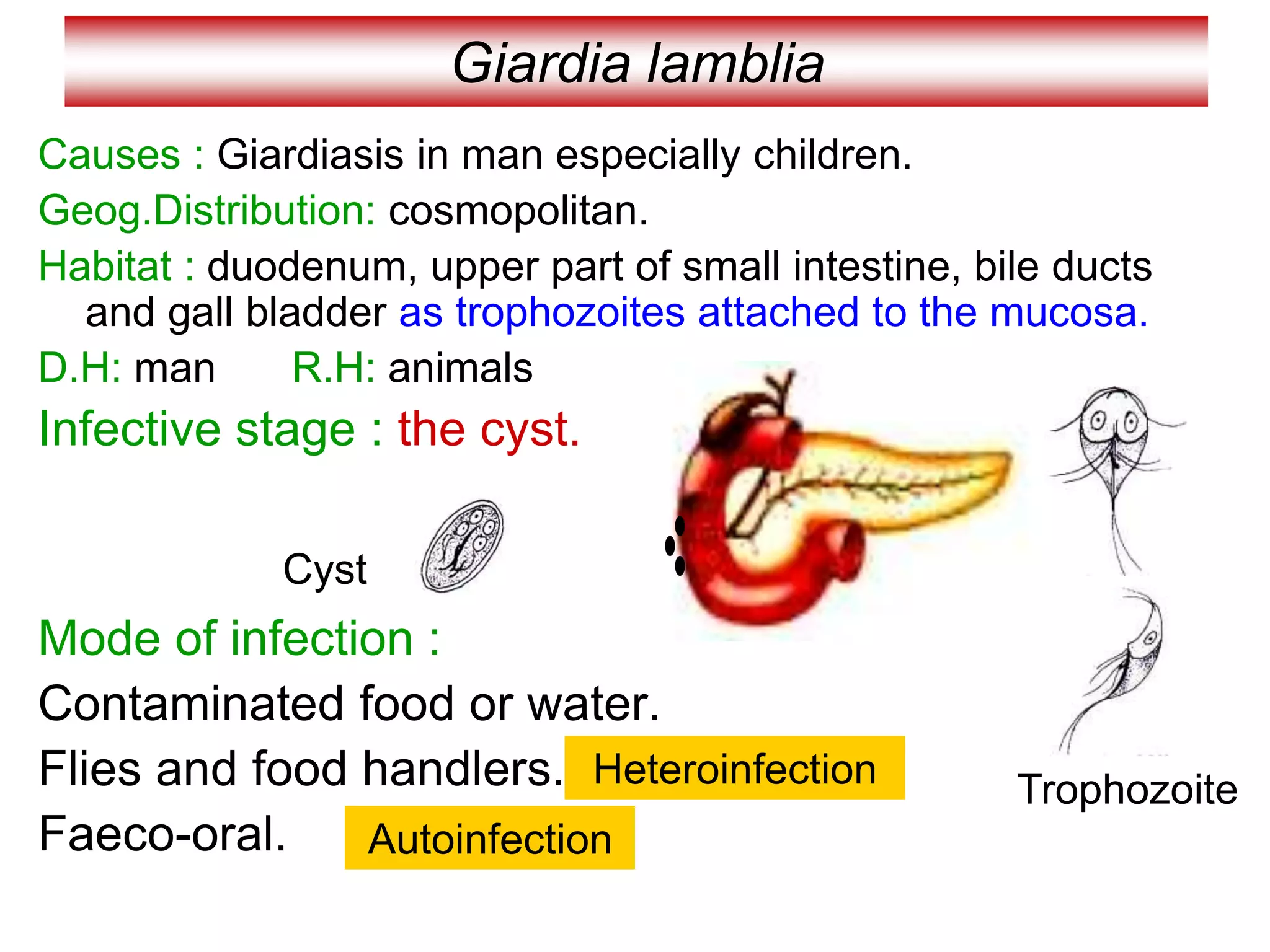
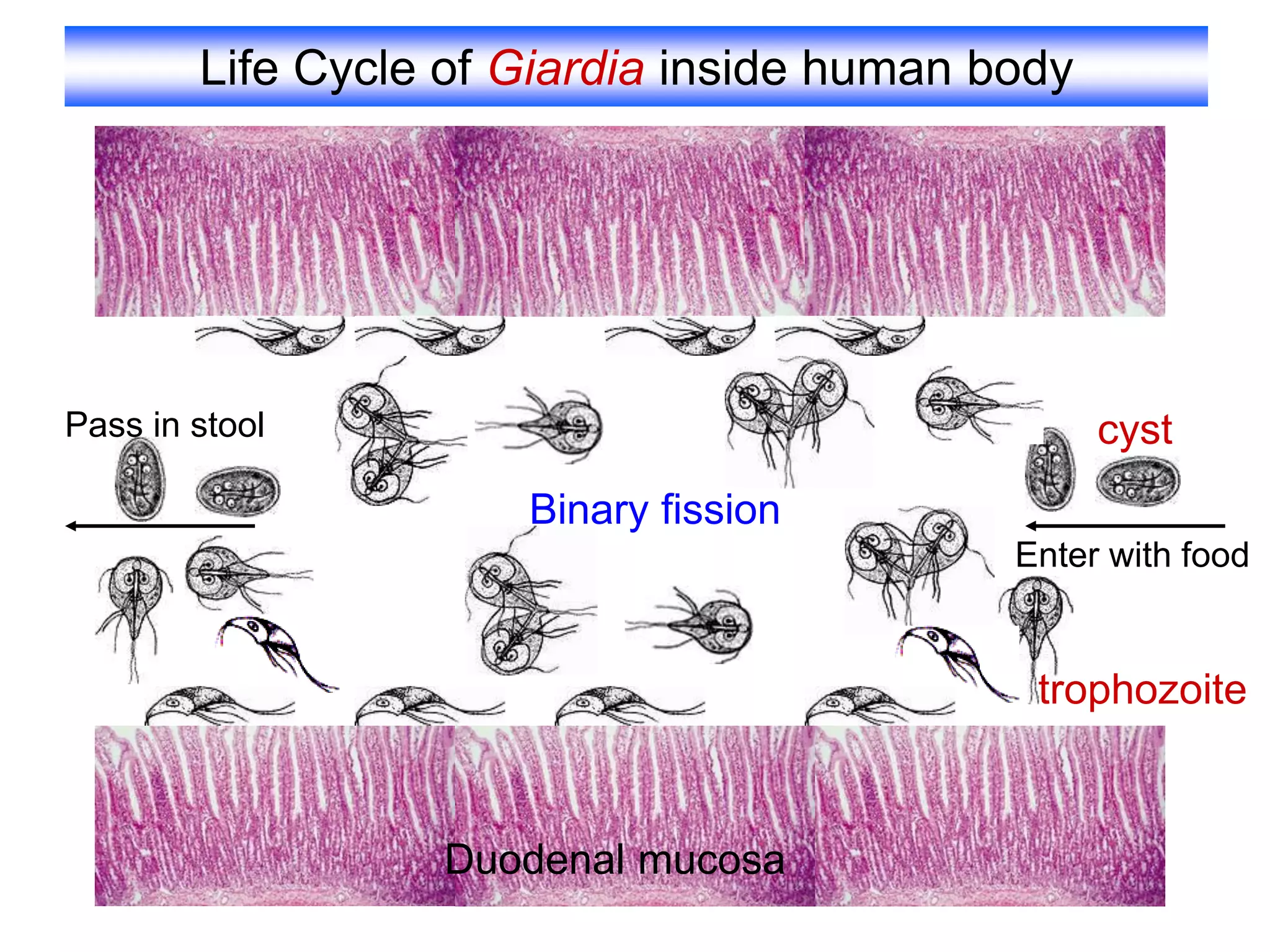
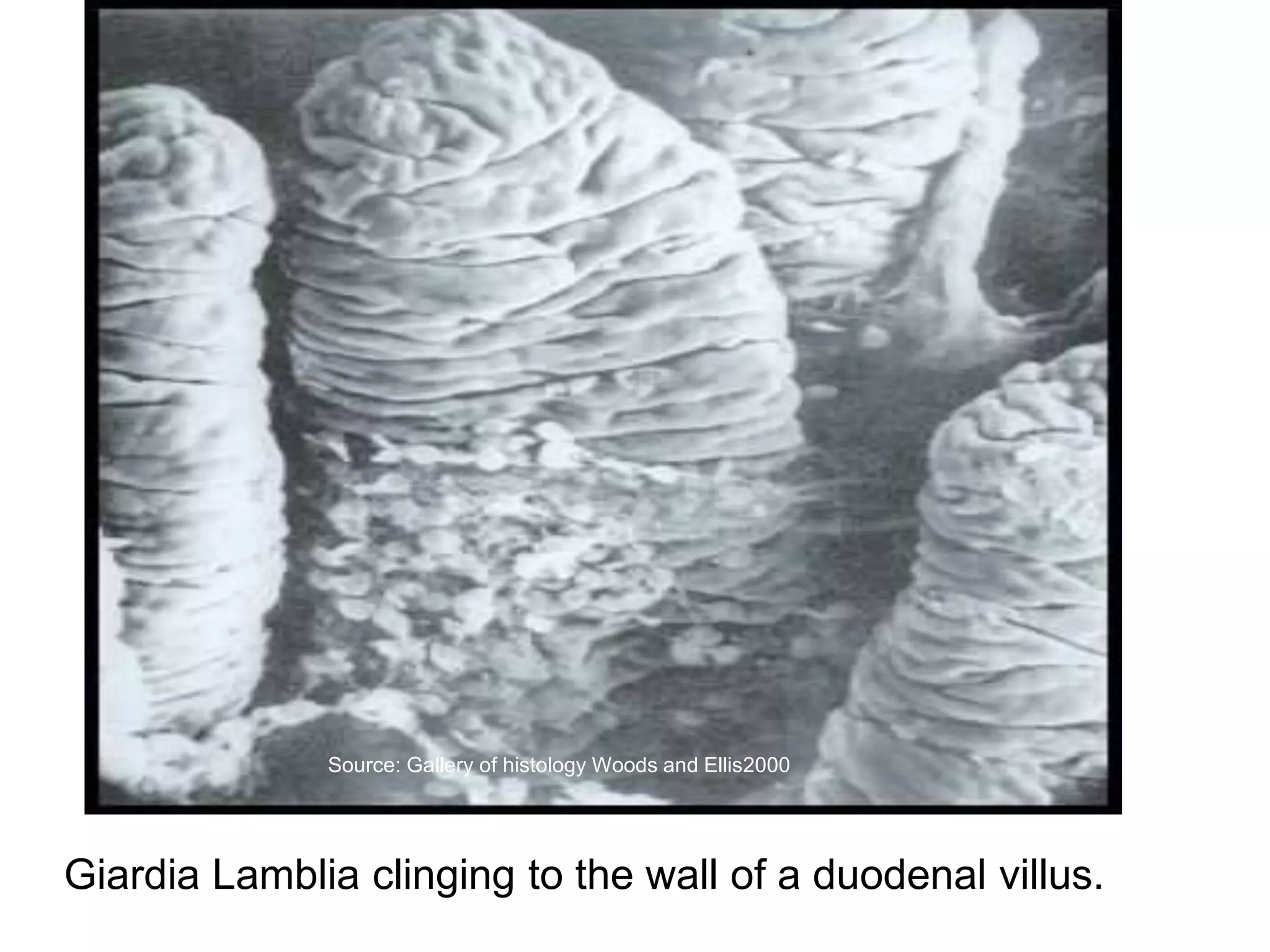
Giardia lamblia is a protozoan parasite that causes giardiasis. It inhabits the duodenum and upper small intestine where it attaches to the mucosa as trophozoites. The infective stage is the cyst, which can be transmitted through contaminated food or water or via person-to-person contact. Symptoms range from asymptomatic carriage to acute diarrhea.














































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)








