Downloaded 443 times

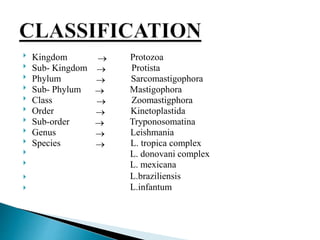
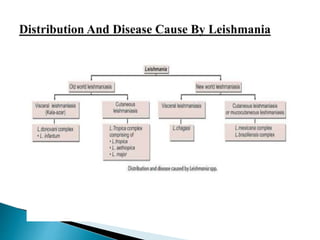

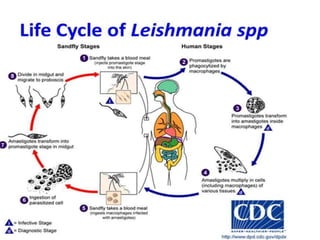




This document describes Leishmania donovani, the parasite that causes visceral leishmaniasis or kala-azar. It discusses the parasite's classification, life cycle within human and sand fly hosts, geographic distribution, morphology in amastigote and promastigote forms, transmission via phlebotomine sand fly bites, pathology in organs like the spleen and liver, clinical features of kala-azar infection, and treatments like liposomal amphotericin B and miltefosine. It also briefly summarizes Leishmania species complexes that cause cutaneous and mucocutaneous leishmaniasis.