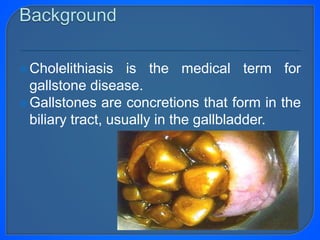
Gallstones are concretions that form in the biliary tract, usually in the gallbladder. Cholelithiasis refers to gallstones in the gallbladder, while choledocholithiasis refers to gallstones in the common bile duct. Treatment depends on whether gallstones are asymptomatic or symptomatic. Asymptomatic gallstones may be managed expectantly, while symptomatic gallstones usually require surgical removal of the gallbladder (cholecystectomy) or other interventions if complications occur.

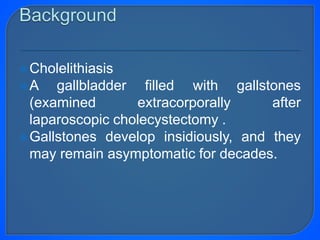
![Obstruction of the pancreatic duct by a
gallstone in the ampulla of Vater also can
trigger activation of pancreatic digestive
enzymes within the pancreas itself, leading
to acute pancreatitis.[1, 2]](https://image.slidesharecdn.com/gallstonediseaseshegazy-180222221357/85/Gall-stone-diseases-hegazy-41-320.jpg)















































![Surgery cholangitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/surgery-cholangitis1-120601032247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







