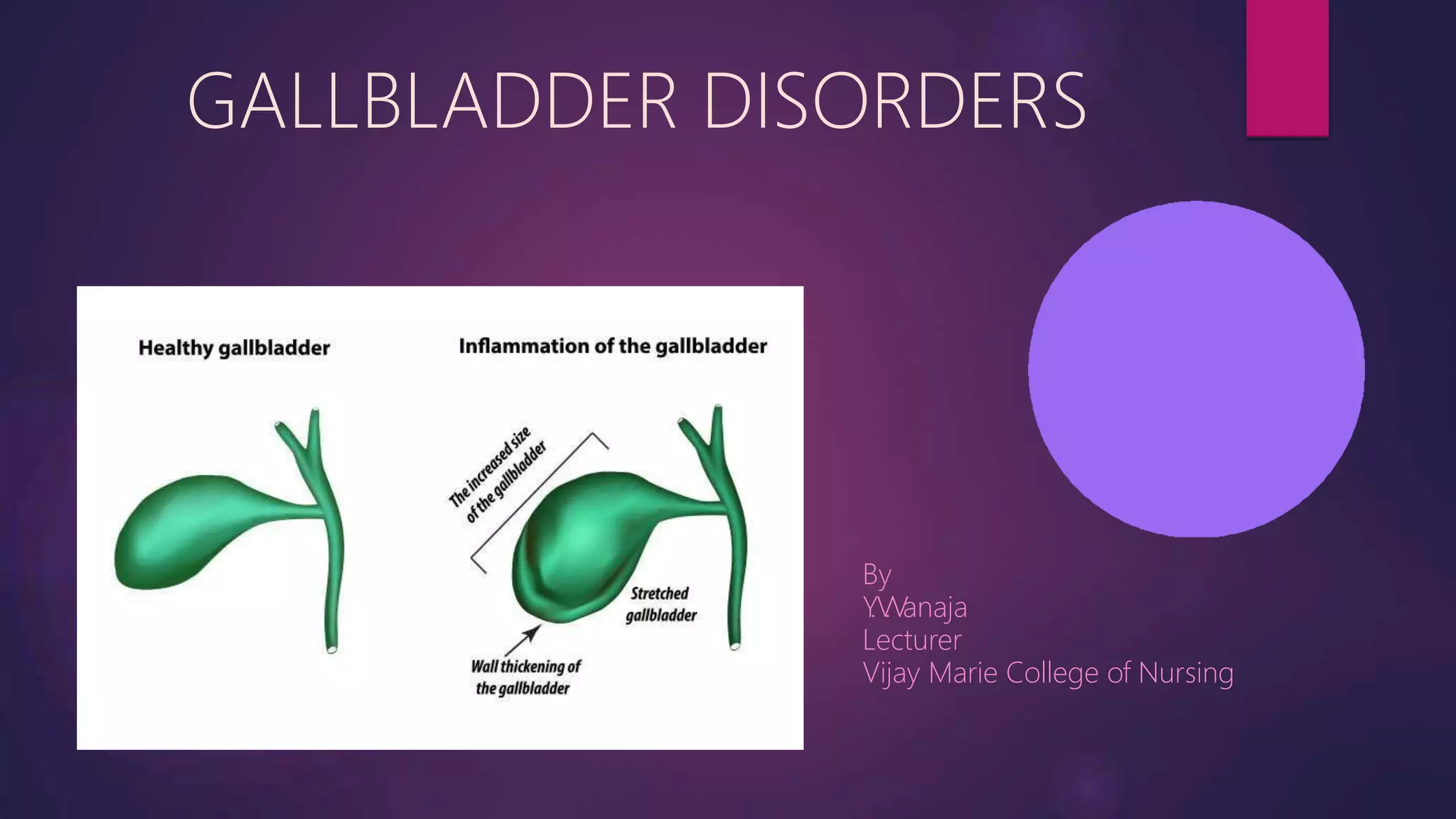
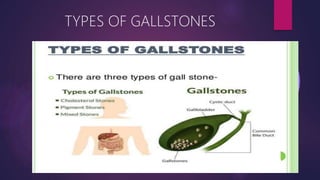
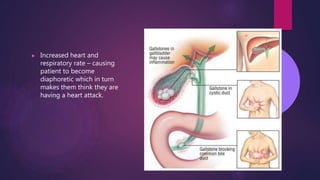
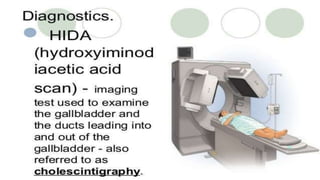
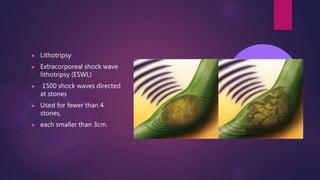
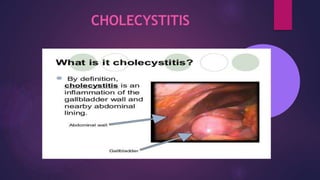
Gallbladder disorders include cholelithiasis, acute cholecystitis, and chronic cholecystitis. Cholelithiasis refers to gallstones, which form from bile constituents like cholesterol and pigment in the gallbladder or bile ducts. Risk factors include age, female sex, obesity, family history, and estrogen therapy. Acute cholecystitis is inflammation of the gallbladder due to gallstones obstructing the cystic duct or gallbladder neck. Symptoms include right upper quadrant pain, nausea, and fever. Chronic cholecystitis results from repeated inflammation and infection leading to gallbladder fibrosis. Treatment involves antibiotics, pain management, and cholecystectomy for severe or recurrent cases










































































![CONGENITAL DIAPHRAGMATIC HERNIA [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/congenitaldiaphragmaticherniarecovered-240421180720-5c4f960f-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

