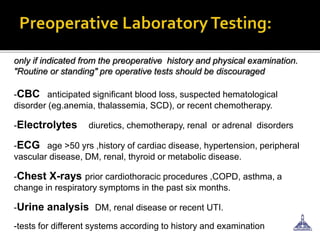
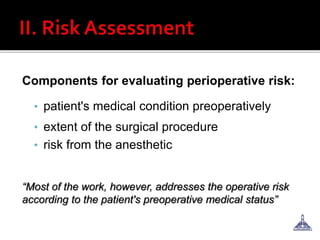
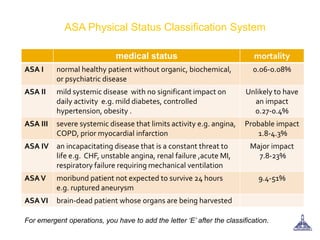
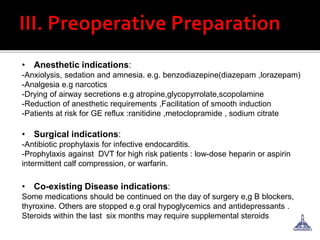
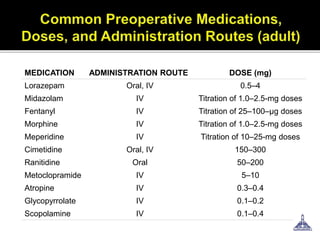
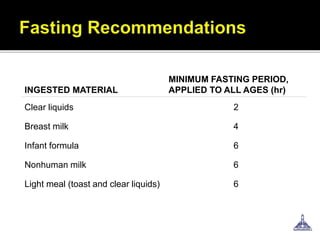
The document provides guidance on preoperative evaluation and optimization of patients for anesthesia and surgery, noting that a thorough review of medical history, physical exam, and any necessary tests should be completed to ensure a patient's medical conditions are addressed and they are in the best possible condition prior to an elective procedure. Factors like airway assessment, cardiovascular and respiratory status, medications, and ASA classification can help evaluate perioperative risk and determine appropriate anesthesia technique and postoperative management.