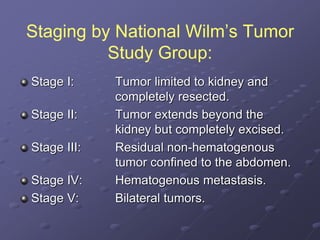
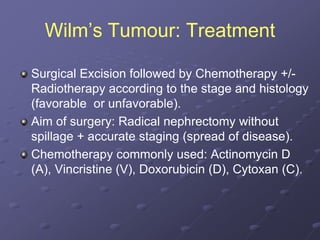
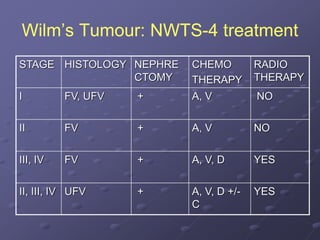
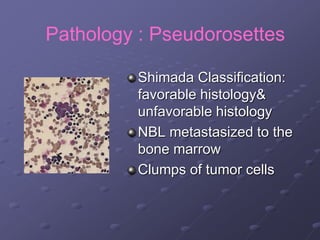
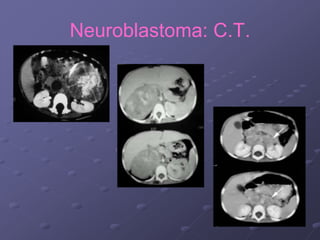
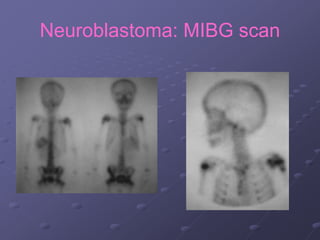
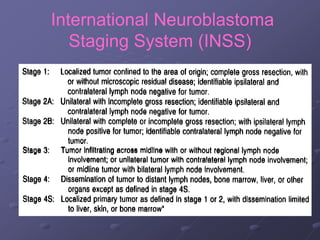
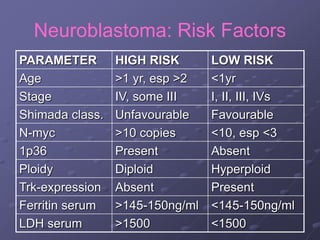
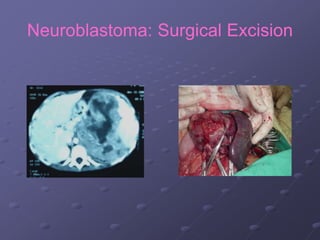
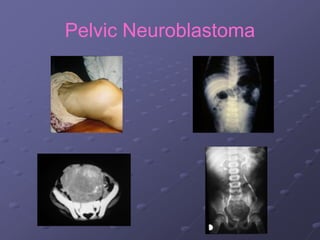
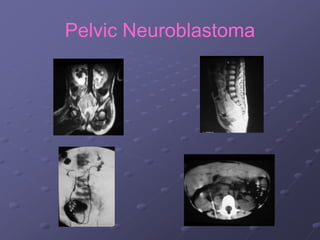
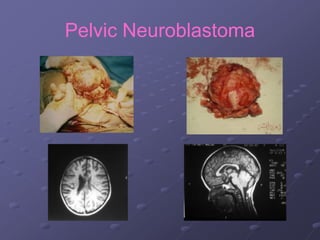
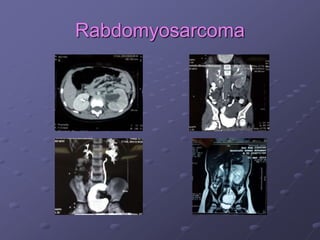
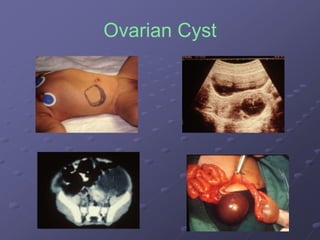
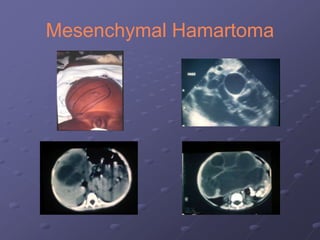
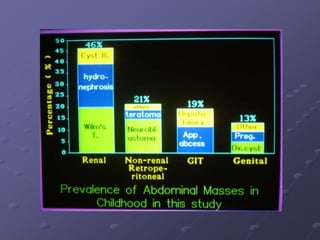
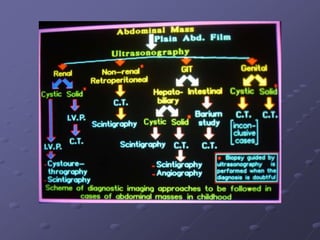
This document discusses and classifies both solid and cystic pediatric abdominal tumors. It provides detailed information on common tumors such as Wilms tumor (nephroblastoma), neuroblastoma, hepatoblastoma, teratoma, intestinal lymphoma, and rabdomyosarcoma. For each tumor, it describes characteristics such as presentation, pathology, imaging findings, staging, and treatment approaches including surgery and chemotherapy. It also covers cystic lesions including hydronephrosis, mesenteric cysts, ovarian cysts, pseudo pancreatic cysts, and liver cysts. The document serves as a comprehensive reference for the diagnosis and management of major pediatric abdominal tumors.


























































![Wilm's tumour - The most common kidney tumor in children - Dr Vishnu A [VCR],...](https://cdn.slidesharecdn.com/ss_thumbnails/vishnu-wilmstumour-210312145616-thumbnail.jpg?width=640&height=640&fit=bounds)














































