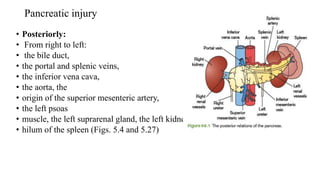
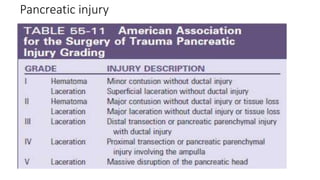
The document discusses pancreatic injuries, highlighting their incidence, mortality rates, and various causes such as road traffic accidents. It outlines diagnostic approaches including imaging techniques and various classification systems for treatment based on injury severity. Additionally, it provides insights into management algorithms, emphasizing non-operative and surgical treatment options along with potential complications.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















