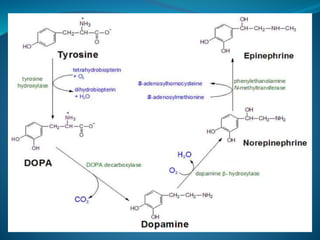
- Pheochromocytoma is a rare tumor of the adrenal medulla that secretes excess catecholamines, leading to episodic headaches, sweating, and tachycardia.
- Diagnosis involves measuring levels of catecholamines and metanephrines in urine or plasma samples. Imaging tests such as CT, MRI, or MIBG scans are also used.
- Treatment begins with alpha-blockade prior to surgery to remove the tumor, followed by long-term use of alpha-blockers or calcium channel blockers to control blood pressure.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















