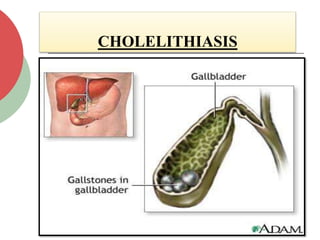
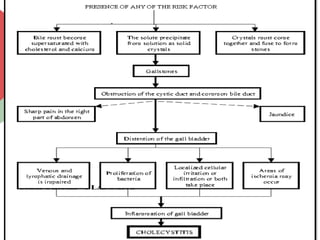
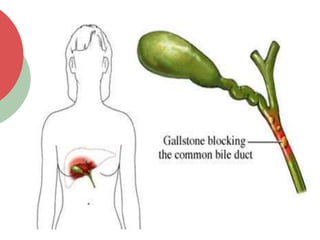
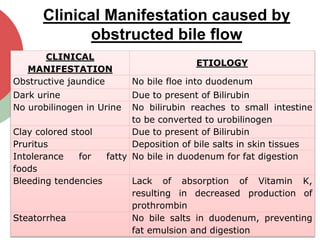
The document discusses cholecystitis and cholelithiasis, conditions related to the gall bladder characterized by inflammation and the presence of gallstones, respectively. Risk factors include gender, age, obesity, and lifestyle choices, while symptoms can range from pain and indigestion to more severe manifestations of obstructed bile flow. Diagnosis typically involves imaging techniques and laboratory tests, with treatment options ranging from conservative management to surgical interventions such as cholecystectomy.