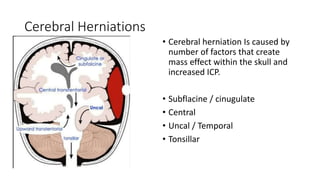
- Cerebral herniation occurs when brain tissue shifts from its normal position inside the skull due to increased intracranial pressure. This is a medical emergency.
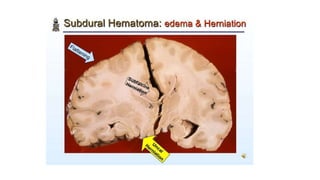
- Common causes are cerebral edema, hematoma, stroke, tumor, and infections.
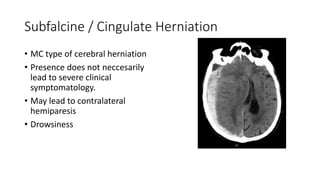
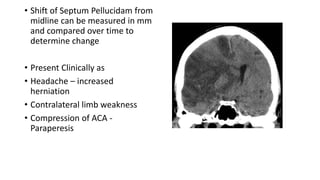
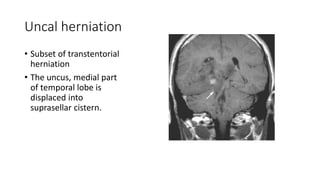
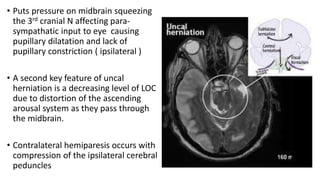
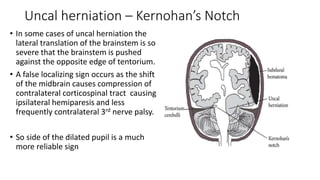
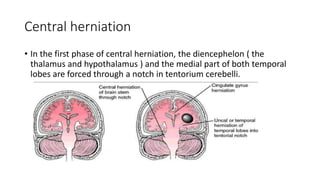
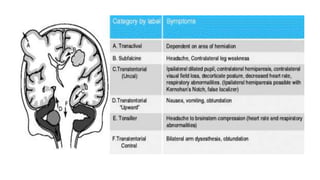
- There are several types of cerebral herniations including subfalcine, central, uncal, and tonsillar. Uncal herniation can cause pupillary dilation and decreased consciousness as it compresses the midbrain.
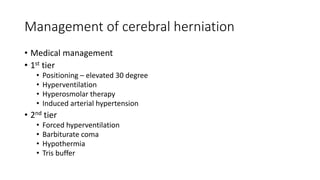
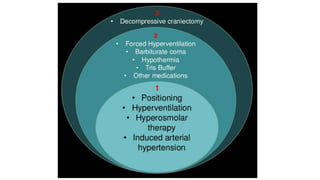
- Increased intracranial pressure can be managed medically with positioning, hyperventilation, hyperosmolar therapy, and induced hypertension or surgically with decompressive craniectomy.